Patient-triggered recording
Tracing
Manufacturer Biotronik
Device ILR
Field Biomonitor
N° 1
Patient
78-year-old man participating in the LBBB-TAVI study.
Graph and trace
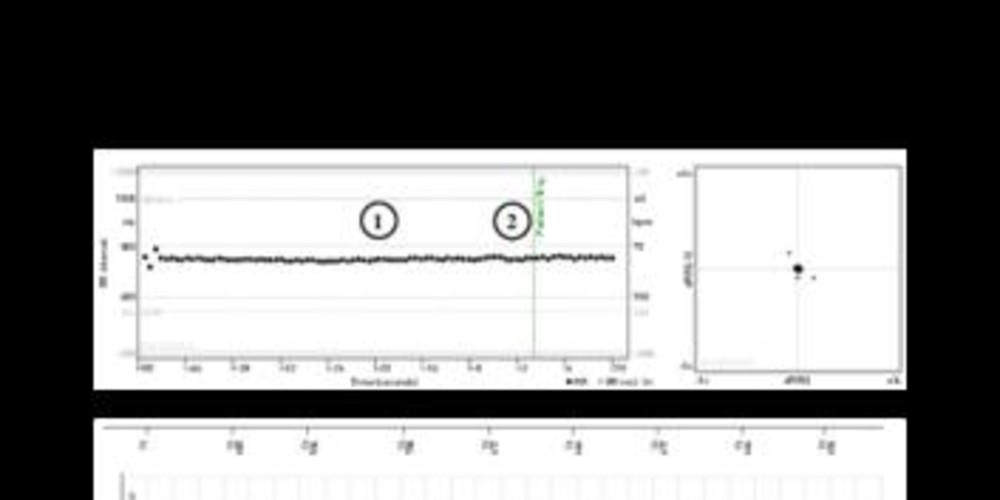
Patient-triggered tracing;
- no change in heart rate throughout the tracing; pattern consistent with a stable sinus rhythm and a heart rate slightly under 90 beats/minute; on the tracing, QRS complexes and T waves are easily identifiable, P waves are of lower amplitude but remain nonetheless visible;
- recording triggered by the patient (50 seconds of tracing prior to activation and 10 seconds thereafter).
Other articles that may be of interest to you


all Biomonitor tracings analyzed in this chapter stem from implanted patients in the setting of the LBBB-TAVI study. Indications for implantation of a TAVI have increased exponentially in recent years. The occurrence of a left bundle branch block furthermore complicates this type of procedure in 5 to 40% of patients and is associated with impaired prognosis in conjunction with an increased risk of atrioventricular block, heart failure, ventricular rhythm disorders and sudden death. Management of these patients varies depending to the centers with more or less aggressive strategies. The main objective of the LBBB-TAVI study was to validate a decision algorithm in patients implanted with a TAVI and presenting a left bundle branch block during follow-up. An electrophysiological study was systematically performed. If the HV interval was prolonged (> 70 ms), a dual-chamber pacemaker was implanted. Otherwise, a BioMonitor implantable loop recorder was positioned and monitored remotely by telemedicine. This explains why in almost all of the tracings presented, the patients present a widened QRS, with the presence of a left bundle branch block being an inclusion criterion. The results of this study are still pending.
The traditional indication of this type of device nonetheless remains the work-up of unexplained syncopes. Indeed, since its introduction some twenty years ago, the implantable loop recorder has positioned itself as a diagnostic tool of reference in this setting. Syncope is a major public health concern, with between 40% and 50% of the general population experiencing an episode of syncope in their lifetime and syncopes accounting for 1-6% of hospital admissions. While the anamnesis, interrogation and clinical examination allow a diagnosis of certainty in a majority of patients with reflex syncopes, the yield of conventional investigations is much less in the setting of cardiac syncopes. The implantable loop recorder is a subcutaneous device positioned in the left subclavian region and allows the loop recording of a bipolar electrocardiographic tracing over a prolonged ambulatory period of time. The device has a rolling memory which records and stores the electrocardiogram after activation by the patient or a witness during the course of a symptomatic episode but can also automatically record electrocardiograms according to pre-programmed sensing criteria. Technological developments, as part of the development of nanotechnologies and telecommunications, has enabled the miniaturization of the monitor and the possibility of remote interrogation.
While the correlation between symptoms experienced by the patient and the electrocardiographic recording represents the gold standard in syncope work-up, it nonetheless remains difficult to obtain with the traditional methods of electrocardiogram monitoring given the sporadic nature of the symptoms. The main objective of the implantable loop recorder is therefore to allow the recording of an electrocardiogram in a contemporaneous manner upon the occurrence of symptoms. The patient assistant, which is a portable battery-powered telemetry device, allows the patient to memorize the traces corresponding to a symptomatic episode. To trigger the recording, the patient must apply the assistant on the skin facing the Biomonitor and then press the button for 3 seconds; the device emits an audible signal and a continuous yellow light appears on the assistant for 3 seconds. If the device has in fact recorded a tracing, a continuous green light emitted for a maximum of 30 seconds indicates proper operation; otherwise, a flashing yellow light indicates the absence of recording. When the patient activates the recording, the device freezes 50 seconds of tracing prior to activation and 10 seconds thereafter.
The diagnosis is made in 3 settings:
This patient had presented syncope in the setting of abdominal pain. The tracing allowed to formally eliminate the diagnosis of conduction disturbance or rhythm disorder to explain the loss of consciousness.