AdaptivCRT algorithm in a patient with a long PR interval
Tracing
Manufacturer Medtronic
Device CRT
Field AV & VV delays optimization
N° 10
Patient
76-year-old man implanted with a triple-chamber defibrillator Viva Quad XT CRT-D for ischemic cardiomyopathy with a left bundle branch block and a long PR interval; follow-up 6 months after implant.
Graph and trace
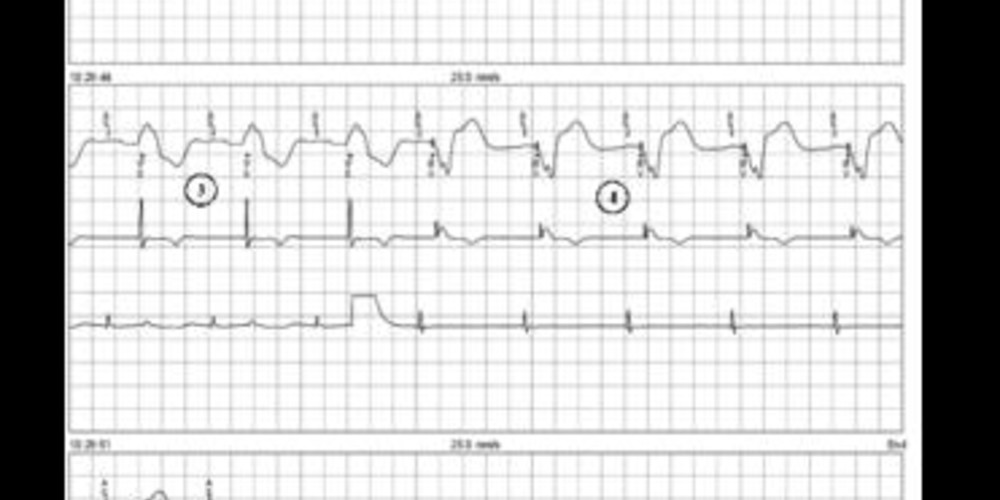
The first line corresponds to an electrocardiographic lead with superimposed markers (MA), the second line corresponds to the bipolar right ventricular EGM (EGM3) and the third line to the bipolar atrial recording (EGM1);
- sinus rhythm and biventricular pacing (AS-BV) without AdaptivCRT function;
- programming of the AdaptivCRT algorithm in Auto Bi-V and LV mode;
- temporary prolongation of the AV delay to 300 ms; 5 AS-VS cycles with a LBBB morphology and a long PR interval; the delay between bipolar atrial EGM and the right ventricular bipolar EGM exceeds 200 ms but lasts less than 300 ms;
- biventricular pacing;
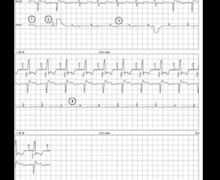
Deprogramming of the AdaptivCRT and reprogramming to the Auto Bi-V mode; - sinus rhythm and biventricular pacing (AS-BV) without the AdaptivCRT function;
- programming of the AdaptivCRT algorithm in Auto Bi-V mode;
- temporary prolongation of the AV delay to 300 ms, 5 consecutive AS-VS cycles with a LBBB pattern and a long PR interval; the delay between the bipolar atrial EGM and the right ventricular bipolar EGM exceeds 200 ms but lasts less than 300 ms;
- biventricular pacing.
Other articles that may be of interest to you

EGM recordings

The various manufacturers offer in their defibrillator or CRT pacemaker platforms, a specific algorithm dedicated to the automatic optimization of the AV and VV delays.
The AdaptivCRT algorithm proposed by MedtronicTM is available with 3 different programming modes:
The Adaptive CRT algorithm is based on regular measurements of (1) the atrioventricular conduction time measured by the leads corresponding to the delay between the EGM sensed by the right atrial lead and the EGM sensed by the right ventricular lead, 2) the width of the P waves corresponding to the delay between the atrial EGM sensed by the atrial bipolar channel and the end of the atrial EGM measured on the defibrillator far-field channel and 3) the width of the QRS complexes corresponding to the delay between the right ventricular EGM sensed by the RV ventricular bipolar channel and the end of the ventricular EGM measured on the far-field channel.
This algorithm never leads to the programming of extreme values (very short AV delay or very long AV delay). The sensed AV delay range for the AdaptivCRT function is between 80 ms and 140 ms (never less than 80 ms or more than 140 ms). The paced AV delay range for the AdaptivCRT function is between 100 ms and 180 ms. The corresponding V-V pacing delay range for the AdaptivCRT function is between 0 ms and 40 ms (left or right pre-excitation).