wave oversensing
Tracing
Manufacturer Biotronik
Device Remote monitoring
Field Periodic Egm
N° 1
Patient
This 47-year-old woman received a single chamber Lumax 340 VR-T ICD after an episode of aborted sudden cardiac death.

Graph and trace
Remote tracings
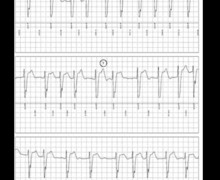
Three channels are available: 1) the markers with the time intervals, 2) the shock channel (FF = far field) between the ventricular lead coil and the can, and 3) the right ventricular (RV) sensing channel with 30 sec of EGM.
- spontaneous rhythm;
- oversensing of a supernumerary signal, probably corresponding to an atrial event; the QRS falls after the PR interval and is classified as VF (PR interval > ventricular blanking programmed at 80 ms);
- intermittent oversensing; alternation of VS and VF cycles, the VF counter is never full and no episode is recorded;
Other articles that may be of interest to you

Systematic oversensing of a supernumerary cardiac signal results from the sensing of 2 signals of different morphologies for a single cardiac cycle. P wave oversensing is likely to occur when the defibrillation electrode of an integrated bipolar lead straddles the tricuspid valve and when the sensed PR interval is longer than ventricular blanking. In this patient, oversensing was intermittent, explaining the absence of an episode stored in the defibrillator memory. P wave oversensing by the ventricular sensing channel may cause the delivery of inappropriate therapies during sinus tachycardia (if the ventricular rate is 120 bpm, the sensed rate is 240 bpm), or during atrial tachycardia. Analysis of the periodic EGM, which was transmitted systematically in absence of alert, allowed an early diagnosis. This patient was seen the morning after reception of this EGM recording. The ventricular lead had to be repositioned in order to eliminate oversensing, by advancing the entire defibrillation electrode inside the right ventricle, as no reprogramming of sensing or of the refractory periods was able to correct the problem.
This tracing illustrates the merits of periodic EGM, which reveal clinical or technical abnormalities that do not fulfill the diagnostic criteria of alert-triggering events, though warrant a medical decision.