Diagnosis alternating between VT and VF zones
Tracing
Manufacturer Abbott
Device ICD
Field Therapy
N° 33
Patient
This 74-year-old man received an AnalyST Accel single chamber ICD for secondary prevention in the context of ischemic cardiomyopathy with syncope. The patient, who was in chronic AF and had undergone His bundle ablation, was seen in routine consultation, complaining of palpitation.
Main programmed parameters
- VF zone at 222 bpm, VT zone at 171 bpm
- 12 cycles in the VF zone and 12 cycles in the VT zone were needed for the diagnosis
- Maximum sensitivity programmed at 0.3 mV
- VF zone: six 36-J shocks (maximum strength); VT zone: 3 bursts followed by 3 ramps of ATP, followed by one 10-J shock, followed by 2 shocks of maximum strength
- Effective discrimination in the VT zone (unnecessary or even harmful in a patient with complete AV block)
- VVI pacing mode at 50 bpm; VVI post-shock pacing mode at 60 bpm
Graph and trace
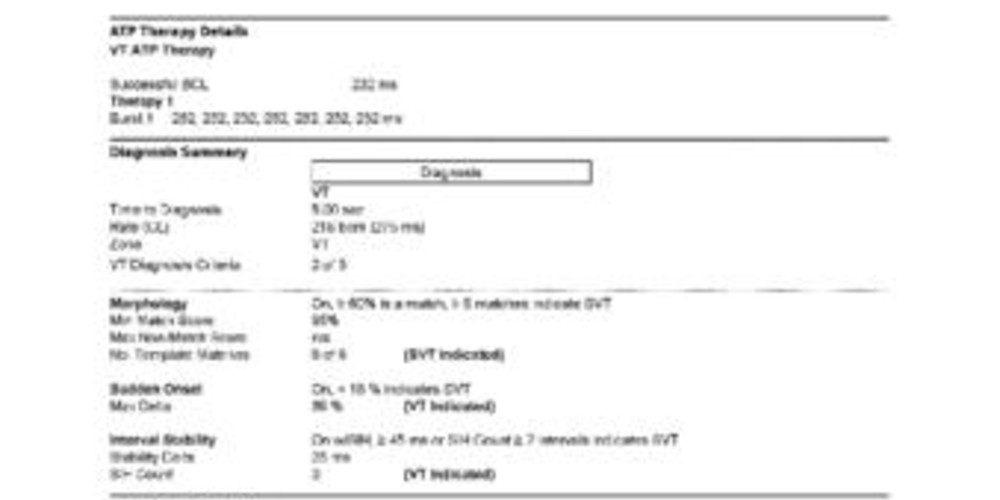
VT episode lasting 12 sec, with burst of ATP appeared to terminate the arrhythmia. The morphology discrimination criterion favours SVT, which is impossible in a patient presenting with complete AV block, highlighting a programming error (no other discrimination than the heart rate in a pacemaker-dependent patient).
Tracing
- Ventricular paced rhythm at the back-up rate of 50 bpm;
- Patient is pacemaker-dependent, VES;
- Onset of VT with unclassified cycles;
- Detection of short cycles in the VF zone;
- Cycles in VT zone;
- Diagnosis of VT after 12 T classified cycles, leaving the VF counter unfilled (7 F instead of 12 needed);
- First therapy in VT zone: burst;
- Successful burst with painless termination of arrhythmia and without energy expenditure.
Other articles that may be of interest to you



In this patient, the tachycardia cycles oscillated between VT and VF zones. The programming of the heart rate range is key in the follow-up of an ICD recipient. This tracing underscores several points: 1) all counters (VT-1, VT-2, VF and return to sinus rhythm) operated simultaneously. The increment of the counter in the fastest zone does not increment the counters in the slower zones. The first counter that reaches the programmed number of cycles determines the detection and the therapies that might have been programmed. In this instance, the VT and VF counters were in competition. The first satisfied was the VT counter, classifying this episode in the VT zone, and prompting the therapies programmed in that zone; 2) the programming of the limit between VT and VF zones has direct repercussions on the discrimination of the arrhythmias. In this patient, the discrimination was active in the VT and inactive in the VF zone, a surprising programming in a patient who had undergone His bundle ablation, was completely pacemaker-dependent, and in whom all rapid ventricular rhythms had to originate from the ventricle; the discrimination should have been deactivated, including in the VT zone, especially since, in this example, the morphology criterion was flawed; 3) various studies have pointed to the merit of programming ATP sequences as first therapy for episodes of fast VT (between 188 and 250 bpm), improving the quality of life compared with the programming of electrical shocks as a first therapy. ATP is successful in 75% of VT in this range of heart rates, without increasing significantly the risk of syncope or acceleration of the tachycardia. In this patient, who developed several like episodes, detection in the VT zone without ATP delivery has prevented the delivery of electrical shocks as a first therapy. The new models of ICD enable the programming of ATP, during or before the charge in the VF zone.