Electrical scalpel
Tracing
Manufacturer Abbott
Device ICD
Field Sensing
N° 24
Patient
A 71-year-old woman recipient of an Atlas dual chamber ICD, implanted for secondary prevention of VT in the context of ischemic cardiomyopathy, was seen for device interrogation a few days after she underwent emergency surgery on the left shoulder. Episodes of VF were recorded that coincided with the time of her operation.
Main programmed parameters
- VF zone at 200 bpm and VT zone at 150 bpm
- 12 cycles in each the VF and VT zones were needed for the diagnosis
- Maximum sensitivity programmed at 0.5 mV
- VF zone: single 30-J shock followed by five 36-J shocks (maximum strength); VT zone: 5 ramps of ATP followed by single 17.5-J shock, followed by single 22.5-J shock, followed by 2 shocks of maximum strength
- Effective discrimination in the VT zone
- DDDR pacing mode at 60 bpm; DDD post-shock pacing mode at 65 bpm
Graph and trace
Narrative
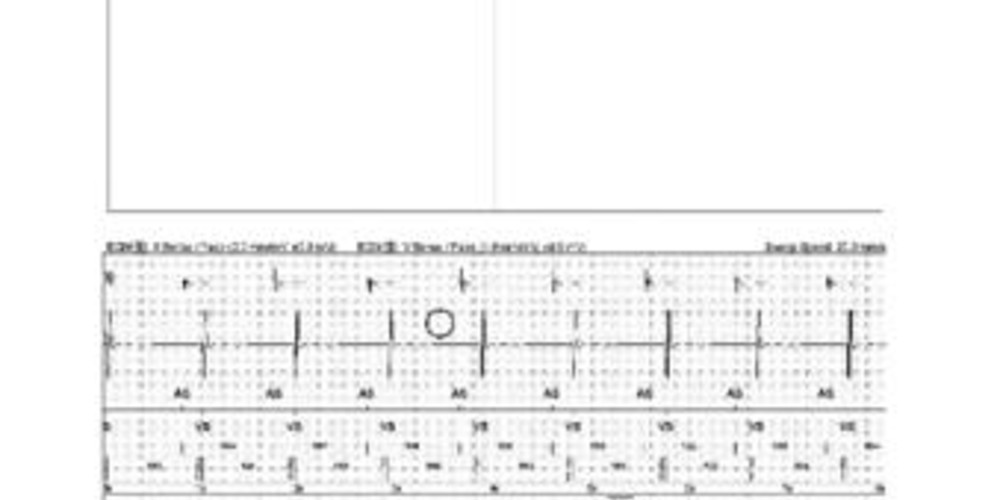
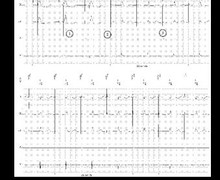
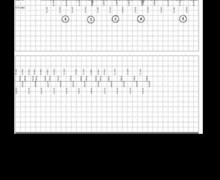
Episode of non-sustained VF with cancelled therapy.
Tracing
1: Sinus rhythm (AS-VS);
2: Sensing of very rapid ventricular signals, variable in amplitude, in the VF zone; absence of concordance between the morphology of these supernumerary signals and the reference EGM morphology; oversensing of disorganized signals in the atrial channel;
3: Diagnosis of VF (12 cycles classified F) and capacitors charge;
4: Intermittent oversensing of very rapid signals in the atrial and ventricular channels, variable in amplitude, during the charge; diagnosis of return of sinus rhythm following the detection of 5 VS cycles; interruption of the charge.
Other articles that may be of interest to you


When an ICD recipient undergoes a surgical intervention, the surgeon must be advised to use electrical scalpels in bipolar mode, to use it for very brief durations, and to place the plates of the scalpel away from the pulse generator.
In order to completely eliminate the risk of dangerous interference, pacing should be programmed to an asynchronous mode, and both detection and therapies should be deactivated. (During periods of therapy deactivation, the patient must be monitored with external defibrillation equipment immediately available.) This is a burdensome strategy, which imposes a preoperative programming as well as a postoperative interrogation of the device, with verification of thresholds and reprogramming. Another option consists of applying a magnet over the pulse generator in order to inhibit all therapy. The magnet also prevents the memorizing of artifactual episodes interpreted as arrhythmias, avoiding the erasure of true arrhythmias occurring before the exposure to interferences, since the rolling memory has a limited capacity. The magnet effect is reversible, and both the therapies and the memorizing of arrhythmias resume upon its removal. During the procedure, surveillance with an oscilloscope is in order, as the patient is no longer protected by the ICD. Finally, the application of a magnet does not preclude a postoperative verification of all ICD functions.