Lead fracture
Tracing
Manufacturer Medtronic
Device ICD
Field Oversensing
N° 25
Patient
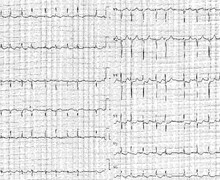
Patient implanted with a triple-chamber ICD (Viva XT CRT-D) not followed in the department, hospitalized for multiple electrical shocks in the absence of prior symptoms; this tracing illustrates a "historical" case of lead fracture.

Graph and trace
- the pacing impedance curve shows a very clear break between normal values followed by a sudden increase with a measurement above 3000 ohms;
- the impedance curve measured in integrated bipolar mode does not show a break in the measurements;
- the right ventricular threshold curve displays a sharp increase in measurements;
- progressive decrease in R-wave amplitude (from 10 to 5 mV); In the device memory, there are initially multiple episodes of non-sustained VT and an episode diagnosed with VF requiring 6 maximum electrical shocks. The graph shows a characteristic scatter plot pattern with high interval-to-interval variability and very short ventricular intervals at the limit of the programmed blanking value. Six maximum electrical shocks are delivered without significant impact on the sensed ventricular rate.
- the EGM is also highly evocative of a lead dysfunction with evidencing of intervals with substantial variability in amplitude and frequency unrelated to the QRS complexes, with some signals saturating the amplifiers and certain intervals at the limit of the programmed blanking.
Other articles that may be of interest to you

This example illustrates the successive steps typically observed during a lead dysfunction. Initially, the device memory reveals multiple episodes of non-sustained VT without anomaly of the lead measurements. In a second step, a clear break can be observed in the different impedance, threshold and right ventricular sensing curves. Finally, the duration of the oversensing episodes is lengthened leading to the occurrence of multiple electrical shocks. This patient had been completely lost to follow up without visual or remote monitoring which precluded early diagnosis; the prevention of inappropriate therapies is one of the major advantages of remote monitoring. This type of episode also demonstrates the value of limiting the therapies to 6 shocks in the VF zone for a single episode. Indeed, the occurrence of successive inappropriate shocks constitutes a particularly difficult and traumatic experience for the patient concerned.
The lead constitutes the weak link of the defibrillation system with a variable percentage of dysfunction depending on the models. When in the presence of a suspected lead fracture, different exams and measurements must be performed: