PR Logic and atrial flutter
Tracing
Manufacturer Medtronic
Device ICD
Field Discrimination
N° 35
Patient
Patient with ischemic cardiomyopathy implanted with a triple-chamber ICD (InSync Sentry); this tracing shows the functioning of the PR Logic algorithm in a patient with atrial flutter.
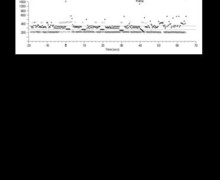
Graph and trace
The graph shows a rapid and regular atrial rhythm and a regular ventricular rhythm; the 2 possible diagnoses are double tachycardia or conducted atrial flutter; no therapy is delivered, the device having concluded to a conducted atrial flutter.
- the EGM shows atrial tachycardia/flutter and rapid ventricular rhythm detected in the VT zone; there appears to be a permanent fixed relationship between atrial activity and ventricular activity (2:1 ratio);
- the device renders the AF/flutter diagnosis when the VT counter is full;
- the FibA / FlutterA option was programmed to ON.
Other articles that may be of interest to you

This patient presented episodes of atrial flutter with 2:1 conduction. This tracing allows detailing the different steps leading to the diagnosis of atrial flutter:
1) is the ventricular rate faster than the atrial rate?
If so, the diagnosis rendered by PR Logic will be VT without further analysis. If, as in the case in point, the atrial rate is faster than the ventricular rate, the analysis continues.
2) is there presence of far-filed R-wave oversensing that could induce an error in the analysis of the atrial rate?
The PR Logic algorithm concludes to an oversensing of the far-field R channel by the atrial channel if it reveals a succession of short interval-long interval atrial sequences and either a short PR interval (<60 ms) or a short AR interval (< 160 ms). In this example, this type of sequences is not found, the PP intervals being perfectly regular (180 ms).
3) is the atrial rate compatible with an atrial arrhythmia?
An AF counter analyzes the number of atrial signals detected between 2 ventricular complexes; when the device shows at least 2 atrial events between two R-waves, the counter is incremented by +1; when the device does not show any atrial event between two R-waves, the counter is decremented by -1; when the device shows one atrial event between two R-waves, the counter is decremented by +1 if the previous cycle was identical (one atrial event between two R-waves); the counter is not changed if the previous cycle was different. The diagnosis of AF is possible if this counter (after correction for possible oversensing) is at minimum +6. In this example, the AF counter increments for each cycle and therefore far exceeds +6. The 3 possible diagnoses at this stage are: conducted AF, conducted flutter and double tachycardia (AF / flutter + VT).
4) is the ventricular rhythm irregular and therefore indicative of a conducted AF?
The analysis of ventricular stability differs from the manner in which stability is assessed with a single-chamber ICD. The device analyzes the RR intervals over 18 consecutive cycles (only the intervals above 240 ms are analyzed) and determines the percentage of cycles observed for a given interval (... 360 ms, 350 ms, 340 ms, 330 ms, 320 ms, 310 ms, 300 ms ...): for example, 35% of the intervals are measured at 360 ms, 27% at 320 ms, etc.
The device sums the percentages of the two most often encountered intervals. If the sum of the 2 percentages is greater than 75%, the rhythm is considered regular. If, on the other hand, the sum is less than 50% (high interval variability), the rhythm is considered as irregular and indicative of a conducted AF. In this example, the rhythm is perfectly stable (360 ms), which allows eliminating the diagnosis of conducted AF. The two possible diagnoses at this stage are: conducted flutter and double tachycardia (AF/flutter + VT).
5) is there an atrioventricular association (conducted flutter) or dissociation (double tachycardia)?
Atrioventricular dissociation is diagnosed if, for at least 4 of the last 8 RR intervals, there is no atrial event or there is a difference of more than 40 ms between the analyzed PR interval and the average of the 8 previous PR intervals. In this example, the PR intervals are perfectly fixed, which explains why the device arrives at the final diagnosis of conducted atrial flutter and therapy is not delivered.
If PR Logic concludes to atrial flutter, Wavelet (if set to ON) is not integrated in the discrimination and therefore cannot change the diagnosis. Conversely, if PR Logic concludes to double tachycardia, Wavelet (if programmed ON) is integrated in the discrimination.