Atrial pacing failure
Tracing
Manufacturer Medtronic
Device PM
Field Pacing & Sensing
N° 15
Patient
72-year-old man implanted with an Adapta dual-chamber pacemaker for sinus dysfunction; programming in AAIRxDDDR mode; reappearance of symptoms typical of lipothymia and fatigue.
Graph and trace
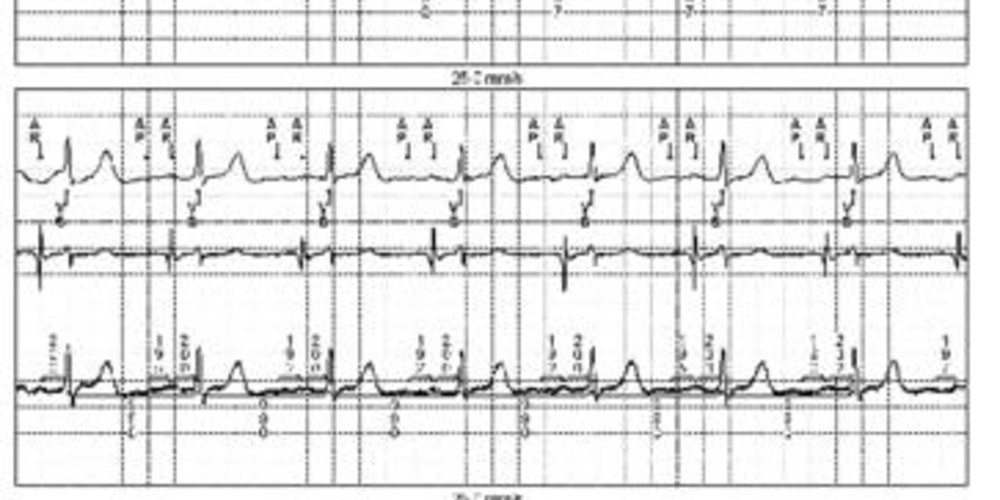
The first line corresponds to lead III with the superimposed markers, the second line to the atrial EGM and the last line to lead II with the superimposed intervals;
- atrial pacing with absence of signs of capture on the atrial EGM; sensing of spontaneous atrial activity labeled AR since occurring in the post-atrial pacing refractory period; spontaneous ventricular conduction (VS);
- continuation of this AP-AR-VS sequence; relative to the beginning of the tracing, the AP-AR interval has progressively increased (162 to 217 ms); in contrast, the AR-VS interval remained fixed (about 200 ms) showing that the spontaneous atrial activity is conducted to the ventricle.
Other articles that may be of interest to you

EGM recordings

This tracing reveals a failure of atrial capture. Atrial output amplitude was programmed in this patient at 2.5 volts for a pulse duration of 0.4 ms. Without an identifiable cause, the pacing threshold had passed beyond this value (threshold at 3 Volts for 0.4 ms). The sensing remained correct (> 2 mV) and the pacing impedance normal (500 ohms). Increasing the output amplitude to 4 volts for 0.4 ms resolved the problem. In a second instance, the pacing threshold stabilized around 1.6 Volts for 0.4 ms allowing long-term programming at 2.8 Volts for 0.4 ms thus ensuring an acceptable safety margin and consumption. This tracing raises the issue of the programming of the automatic adjustment of the atrial pacing amplitude.
As with the ventricular channel, it is possible to program an automatic measurement of the atrial threshold with automatic adjustment of the programming. There are a number of similarities with the functioning of the automatic ventricular threshold but also certain differences. The atrial Auto-threshold model was also favored, the atrial threshold being measured periodically (a single daily measurement at 1:00 am) with the amplitude adjustment as a function of this measurement for the next 24 hours without cycle to cycle verification of capture efficiency. The atrial threshold measurement is not based on the analysis of the evoked atrial response but rather on the highlighting of spontaneous atria or ventricles (2 methods depending on the presence or absence of atrioventricular conduction). Before initiating a pacing threshold search, the pacemaker evaluates whether the patient is paced at the atrial level or whether there is a slow-rate sensing of sinus activity. If the patient's sinus rhythm is normal and stable, the device automatically selects the Atrial Chamber Reset (ACR) method. Otherwise, the device selects the AV conduction method (AVC). Atrial Chamber Reset (ACR) is used to assess the capture by observing the response of the intrinsic rhythm to an atrial pacing that is faster than the spontaneous rhythm of the patient. If the atrial pacing is effective, the sinus activity is inhibited. If the atrial pacing is not effective (absence of capture), the sinus node is not reset, which results in a reappearance of the spontaneous atrial activity. If no spontaneous atrial event is sensed, the device concludes to an effective atrial capture. The diagnosis of loss of capture is thus made on the sensing of spontaneous atrial signals. The AV conduction method (AVC) is applied in patients with preserved AV conduction (1:1 conduction after atrial pacing with fixed AP-VS intervals at a given rate). A loss of atrial capture is demonstrated in the absence of ventricular sensing in the expected window.
Once the threshold measurement is achieved, the device can adapt the output amplitude for the following 24 hours. The minimum pulse duration for the atrial threshold control is 0.4 ms, the maximum amplitude that can be delivered is 5 Volts per 1 ms and the minimum amplitude is 1 Volt for 0.4 ms. This type of programming is therefore not suitable for patients with very high pacing thresholds that can exceed 5 Volts per 1 ms.