Loss of biventricular capture
Tracing
Manufacturer Boston Scientific
Device CRT
Field Left ventricular pacing
N° 8
Patient
This 78-year-old man presenting with chronic AF and complete AV block received a Boston Scientific Autogen triple chamber defibrillator. He was being dialyzed for chronic renal insufficiency and followed by telemedicine.
Graph and trace
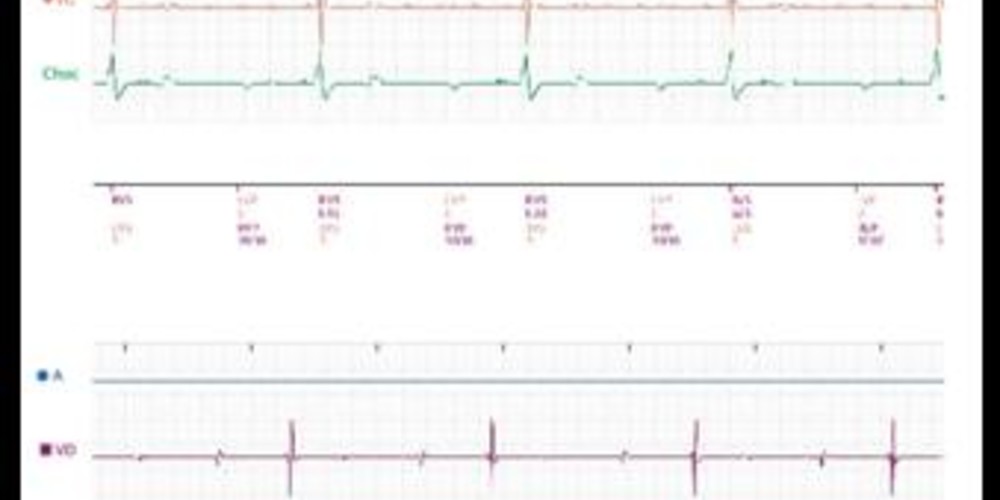
Teletransmission of real time EGM.
- BiV stimulation without capture.
- probable ventricular escape (regular spontaneous rhythm)
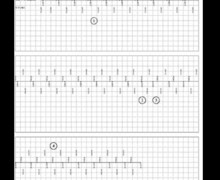
The patient was seen in the ambulatory department and this tracing was recorded. - identical recording of BiV stimulation without capture; ventricular escape
RV pacing threshold - loss of capture at 6.0 V/0.4 ms (6.5 V/0.4 ms threshold). The RV pacing output was programmed at 3.5 V/0.4 ms.
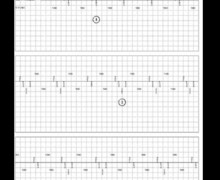
Measurement of LV stimulation threshold in the LV distal – LV proximal programmed configuration. - loss of capture at 3.5 V/0.4 ms (4.0 V/0.4 ms threshold). The LV pacing output was programmed at 3.5 V/0.4 ms.
Measurement of LV stimulation threshold in the LV distal – pulse generator configuration. - loss of capture at 2.1 V/0.4 ms (2.2 V/0.4 ms threshold).
Other articles that may be of interest to you
EGM recordings

This tracing shows a relatively rare increase in threshold on both ventricular leads, explaining the loss of capture. This occurs preferentially in dialyzed patients, in whom wide variations in serum electrolytes occur, particularly in potassium. The follow-up by telemedicine enables a rapid diagnosis, though the remotely transmitted EGM must be analyzed in real-time since the percentage of BiV stimulation may remain high. In this patient, an alert of decrease in the percentage of BiV stimulation was transmitted, after the device had diagnosed ventricular pseudo-bigeminy with alternans of paced and sensed ventricular events. Wide safety margins were programmed to regain effective capture, choosing the LV configuration associated with the lowest threshold.