Alert message for ventricular arrhythmia: episode of classified ventricular fibrillation
Tracing
Manufacturer Biotronik
Device Remote monitoring
Field Messages and events
N° 11
Patient
This 85-year-old man presenting with dilated cardiomyopathy, left bundle branch block and a 25% left ventricular ejection fraction, received a Lumax 540 HF-T triple chamber defibrillator for secondary prevention. He underwent a first device implantation 7 years and pulse generator replacement a few months earlier. He was followed by telecardiology and an alert was transmitted.

Graph and trace
Telemedicine report
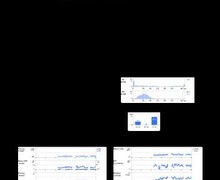
Alert message (yellow status) for episode of classified ventricular fibrillation.
This report indicates that the patient developed an episode of fast ventricular tachycardia (VT) diagnosed in the ventricular fibrillation zone, treated successfully by a sequence of anti-tachycardia pacing. No DC shock was delivered
Other articles that may be of interest to you
EGM recordings
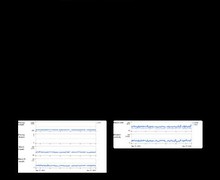
EGM recordings

Telecardiology enables a detailed monitoring of ventricular arrhythmias, and allows the programming of an alert in case of VT in the monitor zone, VT in the VT1 or VT2 zone, ventricular fibrillation, or of successful shock delivery. The EGM allows the verification of the appropriate delivery of therapies. It is noteworthy that the EGM is interrupted at the time of diagnosis and resumes after the delivery of the last therapy. The various therapies and the phase of capacitors charge are not visible.
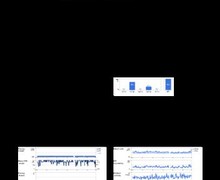
In this patient, anti-tachycardia pacing one shot of this organised VT was successful. This represents an appropriate function of the defibrillator: detection of a ventricular arrhythmia and termination by a painless therapy. The energy consumption was low, since the charge began after the burst of anti-tachycardia pacing and ended as soon as the device diagnosed the return of sinus rhythm.
Since this episode was isolated and asymptomatic, it was not necessary to see the patient in order to change the programming or the medical treatment. On the other hand, if telecardiology detected several such episodes, it would become necessary to see the patient in a face-to-face visit, in an attempt to optimize the medical treatment and, perhaps, offer an ablation of this ventricular arrhythmia. The device programming might also be modified. The ventricular fibrillation zone was relatively wide (starting at 320 ms) and could probably have been narrowed to promote anti-tachycardia pacing therapy of this organized arrhythmia with a single burst in the ventricular fibrillation zone versus several sequences in the VT zone.