Oversensing and connection defect
Tracing
Manufacturer Medtronic
Device ICD
Field Oversensing
N° 28
Patient
Patient implanted with a dual-chamber ICD (Evera XT DR) for hypertrophic cardiomyopathy; the day after implantation, highlighting of non-sustained VT episodes in the device memory in conjunction with a connection defect.
Graph and trace
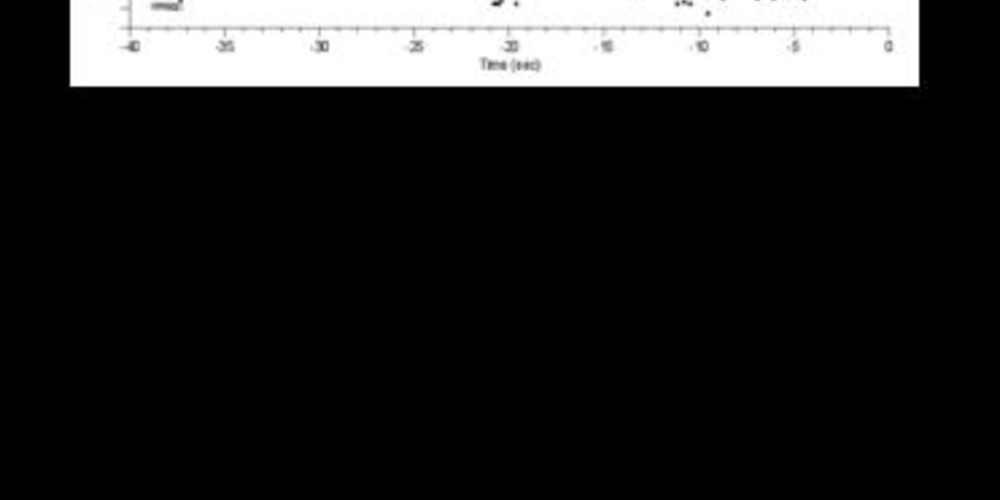
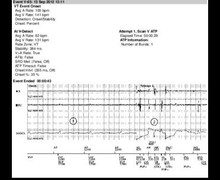
The graph shows a characteristic scatter plot pattern with significant interval to interval variability and very short ventricular cycles at the limit of the programmed blanking value; no delivered therapy and diagnosis of non-sustained VT.
- the EGM reveals intervals with anarchic amplitude and frequency, unrelated to the QRS complexes, with some signals saturating the amplifiers and some intervals at the limit of the programmed blanking.
Other articles that may be of interest to you


When in the presence of inappropriate therapy early after implantation, two causes are to be particularly investigated: faulty connection of the pace/sense pin and an early dislodgement of the ventricular lead. A control interrogation of the ICD allows measuring the pacing thresholds, the R wave amplitude as well as impedances. Lead position can be verified by a chest X-ray.
A connection problem (loosened setscrew connection, incomplete contact between lead pin and header) can yield a similar presentation to that of a lead fracture: the impedance may be abnormally high and the pattern of the EGMs may be relatively similar (fast, disorganized, anarchic and sometimes high-amplitude signals saturating the amplifiers). In such instance, the chest X-ray can confirm the absence of contact between the pin connector and the header. A connector problem is most often revealed within a short time interval after the last intervention (primary implantation or change of pulse generator), the impedance variation and/or the oversensing generally occurring within a few hours to a few days after the procedure. Signs associated with a lead fracture/failure often appear later, except in cases of procedural damage (e.g. direct lesion of the lead with the electric scalpel). In case of a loose connection, manipulating the device inside in the pocket can reproduce the oversensing.
Other atypical presentations may replicate that of a lead dysfunction with combination of an abnormal impedance and oversensing: lead to lead mechanical interaction (contact between the defibrillation lead and a remaining lead fragment or an abandoned right ventricular lead), presence of air in the connector with a specific oversensing pattern corresponding to air bubbles escaping from the connector.
The differentiation between these different clinical situations is essential, albeit sometimes difficult, in order to avoid a false diagnosis of lead fracture which has important therapeutic implications (necessity to replace the lead and discussion on the necessity to extract the "defective" lead). a