Ventricular pacing failure
Tracing
Manufacturer Biotronik
Device PM
Field Pacing
N° 19
Patient
78-year-old man implanted with a Philos II DR-T dual-chamber pacemaker for syncopal complete atrioventricular block; chronic renal failure patient on dialysis; consulting for several episodes of syncope.

Graph and trace
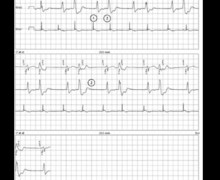
Tracing 19a
- atrial sensing and ventricular pacing with capture;
- atrial sensing and ineffective ventricular pacing.
Patient: 59-year-old man implanted with an Evia DR-T dual-chamber pacemaker for syncope due to sinus dysfunction; routine follow-up control.
Tracing 19b
- effective atrial pacing and ineffective ventricular pacing without capture; unsensed spontaneous ventricular activity since falling within the post-ventricular ventricular refractory period (no possibility of assessing the quality of ventricular sensing on this tracing).
Patient: 61-year-old man, implanted with an Evia DR-T dual-chamber pacemaker for syncope due to paroxysmal atrioventricular block; consulting for repeated lipothymias.
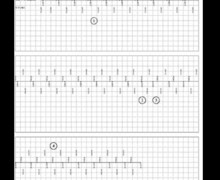
Tracing 19c
- atrial sensing and ventricular sensing (AS-VS);
- blocked P wave, ineffective ventricular pacing without capture.
Other articles that may be of interest to you
EGM recordings


These tracings highlight a loss of permanent or intermittent ventricular capture in patients implanted with a dual-chamber pacemaker. Consequences vary according to the underlying rhythm of the patient. In the first pacemaker-dependent patient with complete atrioventricular block, an intermittent loss of capture (rise in threshold in a dialyzed patient) is associated with the occurrence of syncope and a high risk of sudden death. In the second patient with preserved atrioventricular conduction (implanted for sinus dysfunction), a permanent loss of capture does not cause symptoms. Finally, in the last patient with paroxysmal second-degree atrioventricular block, the loss of ventricular capture is associated with the occurrence of 1- to 2-second pauses due to blocked P wave and responsible for the described lipothymias.
In the presence of a rise in threshold, the question of whether to program the automatic adjustment of pacing output arises. It is therefore important to be completely familiar with the operation of this algorithm and in particular the maximum amplitude that can be delivered in this setting. Indeed, there is a delivered upper limit that does not correspond to the maximum capacities of the device so as to avoid a premature wear of the batteries in the event of algorithm dysfunction. The programming of the automatic amplitude adjustment is therefore not adjusted when the threshold is very high.