Dual chamber discrimination: dual tachycardia, Rhythm ID
Tracing
Manufacturer Boston Scientific
Device ICD
Field Discrimination
N° 4
Patient
This 59-year-old man underwent implantation of a Teligen dual chamber defibrillator in the context of cardiomyopathy due to mitral valve disease and a depressed left ventricular ejection fraction. He presented with episodes of NSVT and chronic AFib and was seen for a routine ambulatory, follow-up visit.
Summary
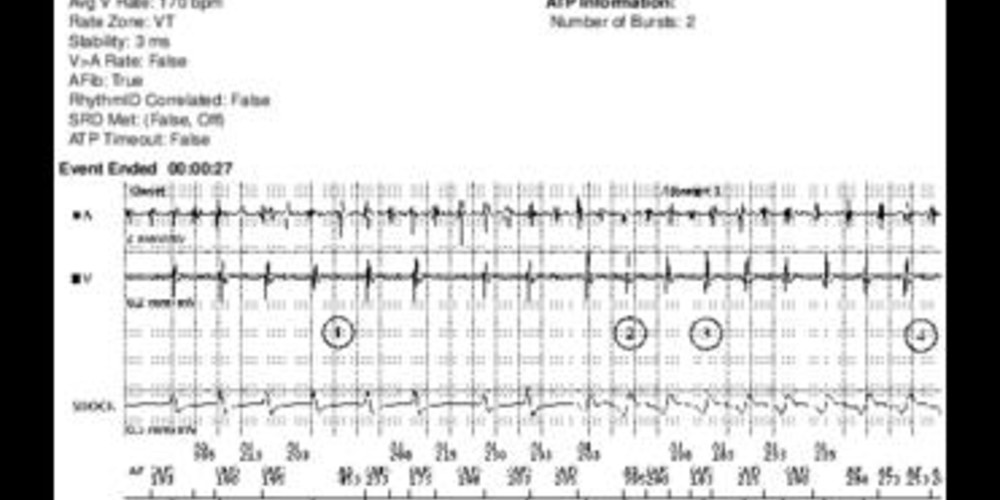
Episode diagnosed as a dual tachycardia (AFib and VT) by the defibrillator; while A is >V, the rhythm is stable and the vectors during tachycardia are unlike the reference vector.
Graph and trace
Tracing
- AFib with relatively rapid and irregular AV conduction;
- sudden acceleration of the ventricular rate with change in the morphology of the ventricular EGM; the rhythm became regular;
- at the third consecutive cycle in the VT zone, onset of the detection of an arrhythmic episode. From this cycle onward, each atrial interval was classified as below or above the AFib threshold, which, in this patient, was programmed at the nominal value of 170 bpm. It is also from this cycle onward (5 cycles before the marker episode) that the measurement of stability began; the mean variance was calculated over these 5 cycles (4 variances);
- after 8 consecutive VT cycles, V-Epsd;
- from this cycle onward, 10 cycles remained until the V-Detect marker. The vectors’ correlation was analyzed during these 10 cycles;
- at the end of Duration, dual tachycardia was diagnosed and the decision was made to deliver therapy: AFib (initially ≥6 out of 10 short atrial cycles followed by the continuation of ≥4 out of 10 short atrial cycles), stable rhythm (measured stability < programmed threshold of stability) without resemblance between morphology during tachycardia and reference morphology (the vector is correlated with the reference vector in <3 cycles out of 10 in the rolling window);
- burst of 10 cycles of ATP;
- apparently unsuccessful burst and persistence of dual tachycardia;
- confirmation of the persistent tachycardia based on the heart rate only (V-Detect);
- second burst of ATP;
- successful burst and termination of the ventricular arrhythmia.
Other articles that may be of interest to you

This tracing illustrates the value of combining discriminators to diagnose complexes tachycardias, such as dual tachycardias. The analysis of AFib Rate Threshold looks for the presence of a rapid atrial rhythm, by comparing the various atrial cycles with a programmed threshold (AFib Rate Threshold). This criterion can only be programmed jointly with Stability. The rationale behind this combination is to inhibit therapy in presence of unstable rhythms with atrial rate > AFib Rate Threshold (suspicion of AFib with atrioventricular conduction).
As in this patient, these 2 discriminators can be combined with the vectors correlation. Under these circumstances, the treatment is:
1) delivered when all discriminators are concordant in favor of VT without AFib (stable rhythm + atrial rate < AFib Rate Threshold + vectors non-correlated),
2) not delivered when all vectors are concordant in favor of AFib and atrioventricular conduction (unstable, atrial rate > AFib Rate Threshold, vectors correlated),
3) delivered for suspicion of dual tachycardia, as in this example (stable rhythm and vectors non-correlated in favor of VT, AFib in favor of dual tachycardia),
4) not delivered for suspicion of AFib with atrioventricular conduction and unreliable atrial sensing (unstable rhythm and vectors correlated in favor of AFib with atrioventricular conduction, though the atrial rate was < AFib Rate Threshold, perhaps revealing the existence of atrial undersensing),
5) not delivered because of suspicion of AFib with aberrant conduction (unstable rhythm with atrial rate > AFib Rate Threshold, in favor of AFib with atrioventricular conduction and vectors non-correlated, in favor of functional bundle branch block),
6) delivered because of suspected unstable VT (vectors non-correlated and atrial rate < AFib Rate Threshold, in favor of VT though unstable rhythm is in favor of unstable VT),
7) not delivered because of suspicion of atrial tachycardia or flutter (vectors correlated, atrial rate > AFib Rate Threshold and stable rhythm in favor of a supraventricular origin with stable and regular AV conduction),
8) not delivered because of suspicion of atrial tachycardia with moderately accelerated atrial rate (vectors correlated and stable rhythm in favor of a supraventricular origin with stable and regular atrioventricular conduction, though the atrial rate is < AFib Rate Threshold, which is fixed at a nominal value of 170 bpm) in favor of an atrial tachycardia that is slower than the programmed threshold.
In summary, when the vectors are correlated, the device inhibits the therapies because of suspicion of SVT with atrioventricular conduction. When the vectors are not correlated, the device delivers the therapies except when the rhythm is unstable and the atrial rate surpasses the AFib Rate Threshold, with a strong suspicion of AFib conducted with aberrancy (functional bundle branch block).