Exercise, anti-PMT algorithm and left ventricular detection
Tracing
Manufacturer Boston Scientific
Device CRT
Field Effort
N° 3
Patient
A 73-year old man with a history of dilated cardiomyopathy and left bundle branch block was implanted with a triple-chamber Boston Scientific Autogen CRT-D. Interrogation revealed a PMT episode.
Graph and trace
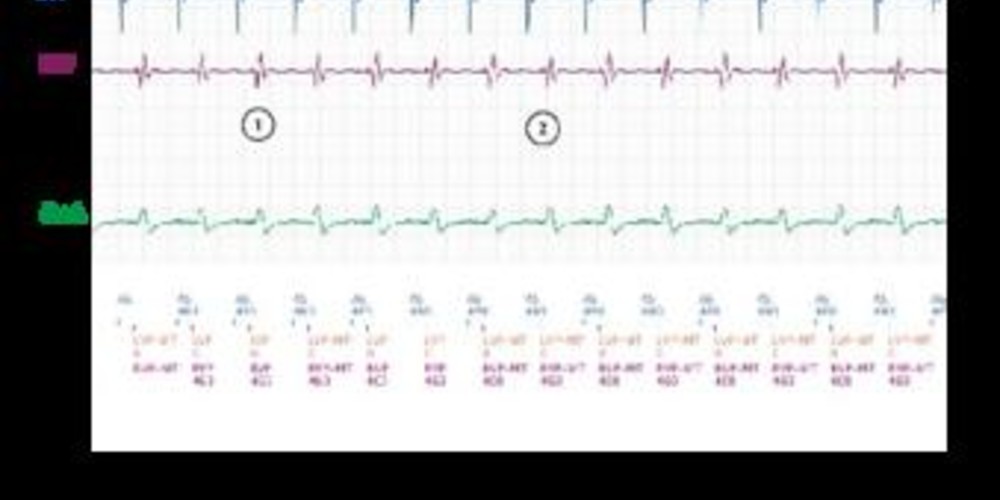
- AS – RVP-LVP cycle during sinus tachycardia.
- AS – VPMT cycle (maximal tracking rate)
- after 16 AS – VPMT cycles, PMT is diagnosed (PMT-B: pacemaker-mediated tachycardia) by the device.
- increase of the PVARP to 500 ms; the atrial activity is detected within the PVARP (AS) which inhibits triggering of an atrioventricular delay (non-conducted P wave); intrinsic conduction with characteristic left bundle branch block appearance (delayed left ventricular activation following right ventricular activation).
- continuation of sinus tachycardia; right ventricular stimulation with long AV delay in order to not surpass the maximal rate; inhibition of left ventricular stimulation since the interval between preceding left ventricular detection and the intended left ventricular stimulation is too short.
- sustained loss of resynchronization with continuation of the same sequence: biventricular detection (RVS-LVS) followed by right ventricular stimulation with inhibition of left ventricular stimulation (RVP-MT – Inh-LVP).
Other articles that may be of interest to you

This EGM shows an example of an anti-PMT algorithm intervention during exercise-induced sinus tachycardia in a patient where the maximal tracking rate has been programmed too low. The final part of the EGM shows a remarkable sustained loss of biventricular stimulation (alternans between right ventricular stimulation and biventricular detection). This episode illustrates the limitations of programming left ventricular detection since it can result in inhibition of left ventricular stimulation. When a premature left ventricular contraction is detected by the right ventricular lead with sufficient delay, left ventricular stimulation could occur within the vulnerable period. This algorithm has been designed to avoid stimulating during this vulnerable period. The downside is that this phenomenon can be result in a loss of resynchronization especially during exercise in patients with left bundle branch block. Tachycardia and delayed left ventricular depolarization during spontaneous activation could lead to isolated right ventricular stimulation on the next cycle while left ventricular pacing is inhibited due to the refractory period.
In this patient, it is necessary to increase the maximum tracking rate. Regarding left ventricular sensing, it is either possible to disable or to decrease the left ventricular refractory period.