Two left ventricular leads
Tracing
Manufacturer Boston Scientific
Device CRT
Field Left ventricular pacing
N° 6
Patient
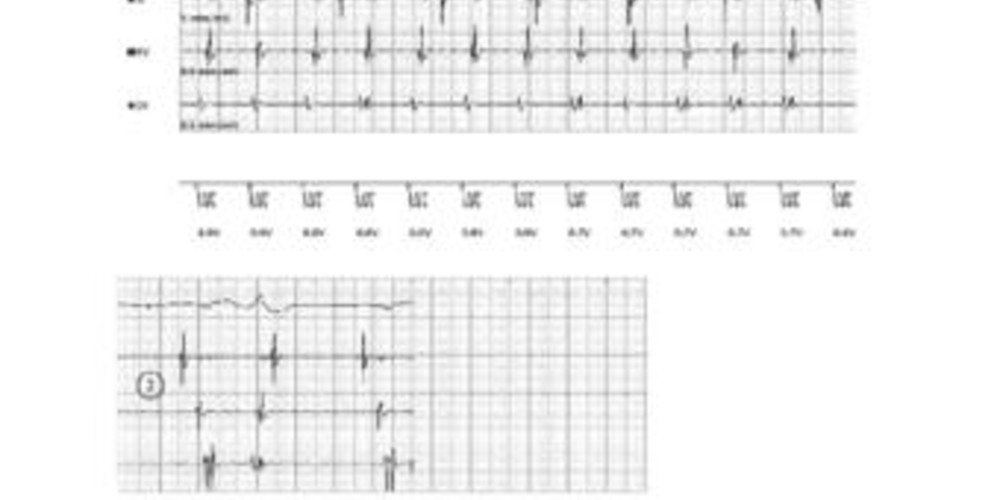
A 62-year old woman implanted with a triple-chamber Boston Scientific Cognis CRT-D connected with 2 left ventricular leads (anterolateral and posterolateral) through a Y-connector with registration of a threshold testing of left ventricular stimulation during different configurations.
Graph and trace
This threshold test is performed with a distal left ventricular electrode to right ventricular anode configuration; VVI mode at 110 bpm.
- Left ventricular capture with alternans between 2 QRS morphologies.
- Loss of capture at a value of 0.6 V.
This threshold test is performed with a distal left ventricular electrode to left ventricular ring configuration; VVI mode at 110 bpm. - left ventricular capture with alternans between 2 QRS morphologies.
- loss of capture at a value of 1.2 V.
This threshold test is performed with a distal left ventricular electrode to can configuration; VVI mode at 110 bpm. - left ventricular capture with alternans between 2 QRS morphologies.
- loss of capture at a value of 0.6 V.
Other articles that may be of interest to you
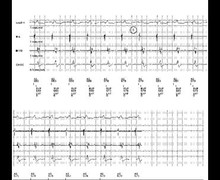



The QRS morphology may vary during left ventricular threshold testing. In VVI mode at 110 bpm, the risk of fusion with native conduction is greatly diminished. Two hypotheses are thus considered: 1) anodal capture or 2) the presence of 2 left ventricular leads connected to a Y-connector. Modifying left ventricular stimulation configurations generally allows for differential diagnostics. The dual QRS morphology is found in the case of anodal stimulation when the configuration includes the coil of the right ventricular lead (identical appearance for distal LV to LV ring and distal LV to can). In contrast, as shown by these EGMs, the dual morphology can be found in all available configurations when 2 left ventricular leads are implanted as long as they have different stimulation thresholds (bi-LV LV morphology and mono-LV morphology). Despite promising early results, the superiority of bi-LV pacing over traditional mono-LV pacing has yet to be demonstrated. The V3 study analyzing the benefits of adding a second LV lead in non-responders was negative. In addition there are technical difficulties limiting the wide-spread applicability (higher risk of complications, anatomical difficulties, Y-connector, …). At the present time, the application in clinical practice for this type of approach remains relatively small.