VF counter
Tracing
Manufacturer Medtronic
Device ICD
Field Counter
N° 1
Patient
Primary implantation of a dual-chamber ICD (Evera XT DR) in a patient with ischemic cardiomyopathy; at the end of the procedure, induction of ventricular arrhythmia by low amplitude electrical shock on the T wave; a single VF zone with a 270 ms limit was programmed (initial detection counter: 12/16); this tracing corresponds to the induction procedure and allows focusing on the functioning of the VF probabilistic counter.
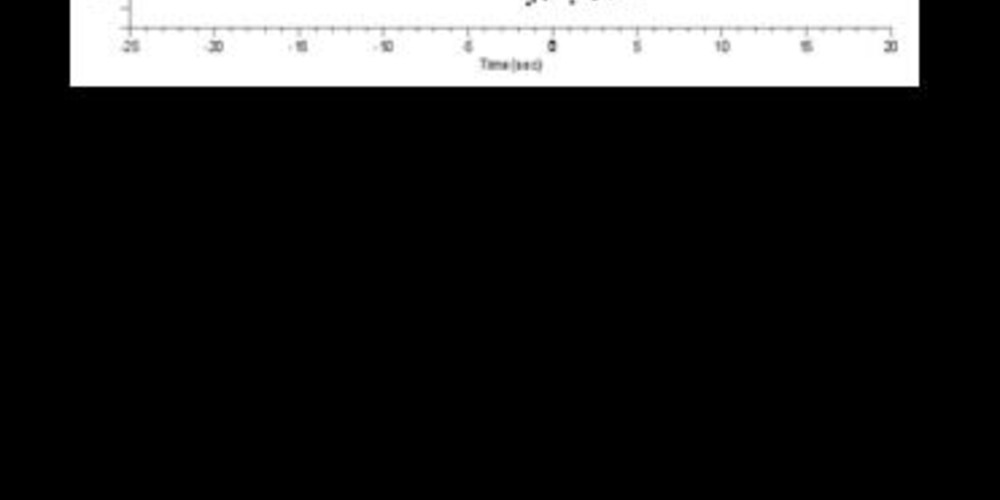
Graph and trace
The graph shows a sinus rhythm followed by rapid ventricular pacing (8 stimuli at 150 beats/minute); the low-amplitude electrical shock delivered on the T wave cannot be visualized on the graph; induction of a probable rapid ventricular arrhythmia detected in the VF zone; highlighting of a few intervals falling outside the VF zone suggesting ventricular undersensing; detection of VF followed by electrical shock of 25 Joules terminating the arrhythmia.
- the EGM initially shows atrial and ventricular pacing;
- rapid ventricular pacing;
- low-amplitude electrical shock delivered on the T wave (320 ms coupling interval); following the shock, blanking period with no possible sensing for 520 ms;
- induction of a rapid and polymorphic ventricular arrhythmia;
- undersensing of a secondary ventricular interval with high variability in signal amplitude; the ensuing interval is classified as VS (long pseudo-interval);
- new undersensing;
- the VF probabilistic counter is filled (programmed at 12/16) with detection of a VF episode and start of the capacitor charge;
- during the charging period, all intervals are classified as VS even when fast and corresponding to the VF zone;
- end of charge and confirmation phase;
- delivered electrical shock; successful electrical shock and end of episode after 8 consecutive intervals classified as VS or VP.
Other articles that may be of interest to you


This tracing allows detailing the functional operation of the VF counter in MedtronicTM devices. It is a probabilistic counter (fast X/Y intervals) which requires a minimum of 75% fast intervals (programming possibilities: 9/12, 12/16, 18/24, 24/32, 30/40, etc). A ventricular fibrillation is, by definition, an arrhythmia that is fast, disorganized, chaotic, with ventricular signals of low and/or variable amplitude. All of these characteristics increase the risk of undersensing with occasional signals with amplitude below the detection threshold (nominal value of 0.3 mV) and often a high variability in beat-to-beat amplitude, which is problematic given that, the device uses a sensitivity level which adapts to the amplitude of the preceding signal. This 75% ratio between fast and slow intervals was chosen so as to obtain an optimal balance between the proper detection of ventricular fibrillation (necessary tolerance for a certain number of long pseudo-intervals generated by undersensing) and the need to not fill the counters in the presence of an oversensing of T, P or R waves (frequently associated with a 50% ratio of short intervals.