difference in sensed AV delay and paced AV delay
Tracing
Manufacturer Abbott
Device PM
Field AV delays, refractory periods management of tachycardia
N° 24
Patient
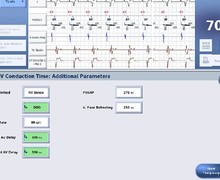
72-year-old man implanted with an AccentTM DR pacemaker for complete atrioventricular block; recording of this tracing during the consultation.
Graph and trace
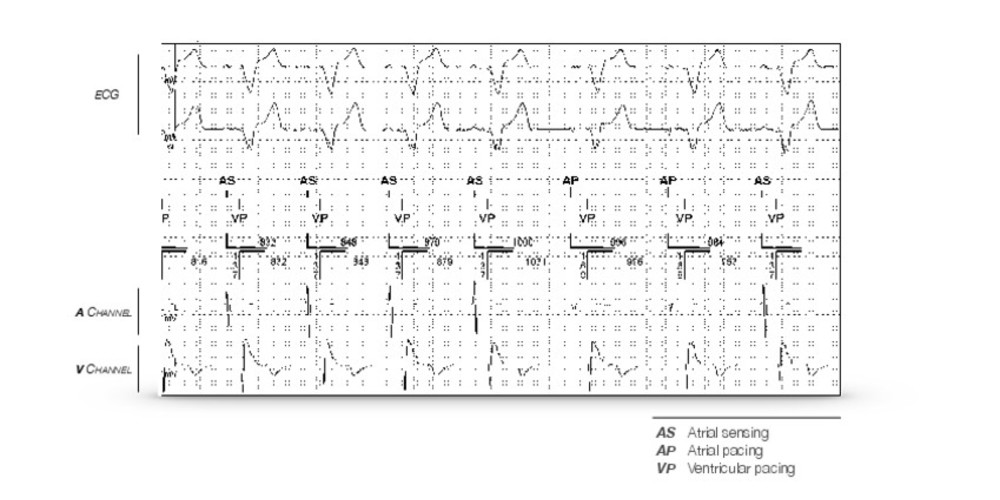
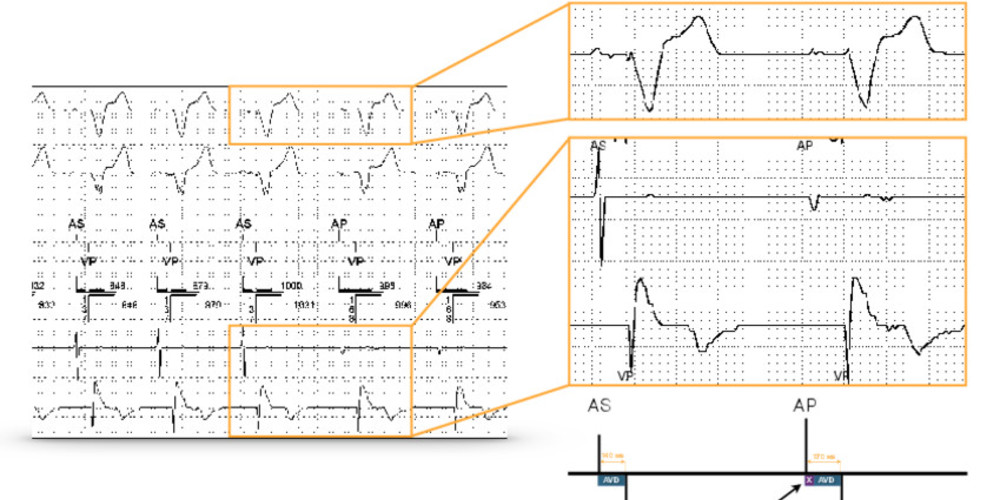
Permanent ventricular pacing; alternation between AS-VP (intrinsic atrium) and AP-VP (paced atrium) cycles; AV delay on paced atrium (170 ms) longer than sensed atrium (140 ms).
Other articles that may be of interest to you

As in this example, the paced atrial AV delay is usually programmed longer than the sensed atrial AV delay for various reasons: the P wave is never sensed at the very beginning of the surface P wave, but rather at the passage of the atrial depolarization wave under the electrode. It is often late comparatively to the beginning of the P wave of the surface ECG. Moreover, when the P wave is paced, the conduction time between the right atrium and the left atrium is prolonged. The difference between sensed and paced AV delays is contingent on the position of the lead in the right atrium: on average 30 ms if the lead is septal, 50 ms if positioned in the appendage, 70 ms if low lateral. These values represent averages and it is theoretically necessary to adjust the programming to each individual. These differences are often greater if there is presence of an intra- and/or interatrial conductive disorder. This difference changes little during exercise, with a tendency to shorten under the influence of catecholamines which reduces the interatrial conduction time. If there is a major interatrial conductive disorder, this difference may be greater during exercise. In practice, this value can remain fixed throughout the variation range of the programmed rate.
Physiologically, the PR interval is shortened during exercise, averaging 4 ms for every 10-beat rate acceleration. The adjustment of the AV delay is designed to reproduce this physiological phenomenon, and the same variation is applied to the sensed AV delay and the paced AV delay. The shortened sensed AV delays during exercise increase the sensing window for detecting rapid atrial events by shortening the total atrial refractory period and increasing the rate of appearance of a 2:1 block. The dynamic AV delay adjusts the AV delays linearly as the heart rate increases. It is possible to program 3 levels of AV delay adjustment according to the heart rate: low (shortening of the AV delay by 0.5 ms for a rate increase of 1 beat/minute), medium (shortening of the AV delay by 0.75 ms for a rate increase of 1 beat/minute) and high (shortening of the AV delay by 1.0 ms for a rate increase of 1 beat/minute). The shortening of the AV delay continues until the heart rate reaches the maximum sensor rate or the maximum synchronous rate or if the AV delay value reaches the value of the shortest programmed AV delay.