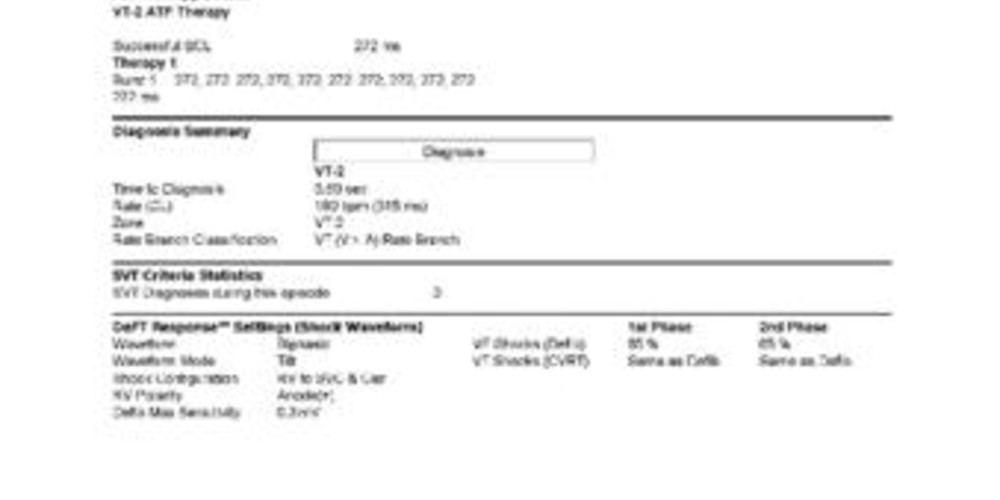
Successful burst of ATP for repetitive episodes of VT
Tracing
Manufacturer Abbott
Device ICD
Field Therapy
N° 30
Patient
This 74-year-old man presenting with ischemic cardiomyopathy, 25% left ventricular ejection fraction, in New York Heart Association functional class III, and left bundle branch block, received a Promote triple chamber CRT-D and was seen on a routine visit.
Main programmed parameters
- VF zone at 222 bpm, VT-2 zone at 181 bpm and VT-1 zone at 160 bpm
- 12 cycles in the VF or VT-1 or VT-2 zones were needed for the diagnosis
- Sensitivity programmed at 0.3 mV
- VF zone: six 36-J shocks (maximum amplitude); VT-2 zone: 2 bursts of ATP, followed by single 10-J shock, followed by highest energy shocks; VT-1 zone: 4 ramps of ATP followed by single 10-J shock, followed by highest energy shocks
- DDDR pacing mode at 65 bpm; biventricular stimulation; DDI episode pacing mode DDD post-shock pacing mode at 60 bpm
Graph and trace
Narrative
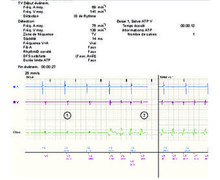
Episode of VT at 190 bpm diagnosed in the VT-2 zone and V>A arm; burst of 12 complexes at fixed rate; post-ATP cycle length at 815 ms; therefore, the therapy was a priori effective.
Tracing
- Atrial sensed and biventricular paced (AS-BP) rhythm;
- VES;
- Initial cycles of the tachycardia were unclassified;
- DDI episode pacing mode after 3 cycles classified T2;
- Fast VT in zone 2 (T2) with AV dissociation (V>A arm);
- Burst of 12 stimuli;
- Post-pacing blanking;
- Successful burst and diagnosis of restoration of sinus rhythm.
Narrative
Another nearly identical episode a few days later.
Tracing
- Fast VT in zone 2 (T2);
- Burst of ATP;
- Successful burst.
Narrative
Another nearly identical episode 2 months later.
Tracing
- Fast VT in zone 2 (T2);
- Burst of ATP;
- Successful burst.
Other articles that may be of interest to you


The defibrillator memory had stored multiples episodes of monomorphic VT at 190 bpm, diagnosed in the VT-2 zone, all successfully treated by a salvo of ATP, preventing repetitive electrical shocks, which would have considerably degraded this patient’s quality of life.
The programming of 2 tachycardia zones allows the differential treatment of tachycardias at different heart rate. In the VT-1 zone, which includes tachycardias at rates below 170 bpm, different sequences of ATP are usually programmed (1 series of 3 to 5 bursts corresponding to salvos of pacing at a fixed heart rate, followed by a series of 3 to 5 ramps corresponding to more aggressive salvos with a programmable decrement from one pacing cycle to the next) before the programming of a series of electrical shocks. For tachycardias detected between 190 bpm and the VF zone, it might be efficient to program a VT-2 zone which includes a more limited number of ATP sequences, with a view to avoid shock therapy as a first choice, while not excessively delaying the delivery of shocks for fast arrhythmias, which can compromise the hemodynamic status if ATP is unsuccessful.