Reveal Linq in a patient with Brugada syndrome
Tracing
Manufacturer Medtronic
Device ILR
Field Reveal Linq
N° 16
Patient
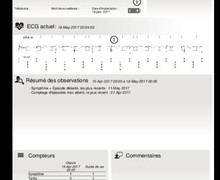
A 22-year-old patient with an electrocardiogram characteristic of Brugada syndrome (type 1) and repeated syncopes of systematic vagal origin; implantation of a Reveal Linq; after his return home, episode of syncope with marked prodromes; recording triggered by the patient.
Graph and trace
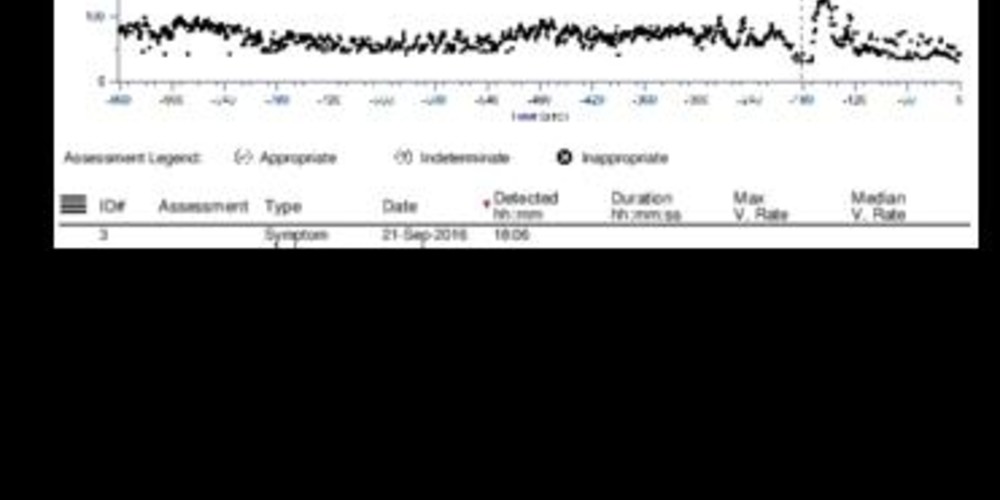
There are 2 recordings for the same episode (1 symptomatic episode triggered by the patient, 1 automatic episode in conjunction with the occurrence of a pause).
- the graph and tracing show a very marked bradycardia with difficulty in differentiating full AV block and sinus pause which would allow validating the pause criterion;
- bradycardia followed by sinus tachycardia;
- "Symptom" marker corresponding to the moment the patient activates the recording;
- upon analysis of the tracing with the markers, the device diagnoses a pause (AD) after an interval of more than 3 seconds without detection;
- the Pause episode ends after occurrence of 12 detected ventricular events.
Other articles that may be of interest to you



The recording of this tracing allows eliminating a tachyarrhythmic origin of the syncope with a very evocative pattern of a vagal origin. One of the improvements in the new implantable Holter platform (Reveal Lnq) is the increased storage capacity. In total, 57 minutes of recording can be stored with:
The device can automatically record 4 episode types: Tachy, Brady, Pause, AT/AF.
In order for an episode classified as Tachy to be recorded, the interval in Tachy must be shorter than the programmed interval (Interval) over a number of cycles at least equal to that programmed (Duration). In addition, very fast rates cause a Tachy episode to be recorded when 30 of the last 40 ventricular events display an interval < 260 ms. If the device shows very short intervals (<220 ms) with a very high frequency of recorded signals (number of times the signal crosses the baseline), it rejects the diagnosis of tachycardia on suspicion of the presence of noise (no episode stored in memory). The Tachy episode ends when one of the following criteria is met:
A bradycardia episode is identified when a programmable number of RR intervals is greater than a determined length (programmable). The bradycardia episode ends when one of the following criteria is met:
The device detects a Pause (asystole) episode when the interval between 2 detected complexes exceeds the duration of the programmed pause (1.5, 3 or 4.5 seconds). The pause diagnosis is rejected if the device suspects an undersensing. When the sensitivity is programmed to 0.025 mV, 0.035 mV or 0.050 mV, a "Loss of signal" counter is incremented with each sensing of an R-wave of amplitude less than twice the programmed sensitivity, and is decremented if the Signal amplitude is greater. If the "Loss of Signal" counter is> 0 on the Vs beat before the pause is detected, the episode is rejected. A Pause episode ends after 12 detected ventricular events.
The device detects the occurrence of AT (atrial tachycardia)/AF (atrial fibrillation) episodes based on changes in ventricular rhythm using an automatic algorithm based on the sequence of variability of RR intervals during 2-minute periods. The difference between the consecutive RR intervals is plotted on a Lorenz curve. The difference between two consecutive RR intervals (ΔRRn) is plotted on the vertical axis while the difference between the previous RR intervals (ΔRRn-1) is plotted on the horizontal axis.
During an AF episode, the RR intervals are extremely irregular and uncorrelated whereas the RR interval sequences are more regular in an AT episode. The occurrence of frequent atrial or ventricular extrasystoles may cause an inappropriate recording of AF-diagnosed episodes in conjunction with a significant variability in RR cycles. Two specific algorithms can limit the number of inappropriate recordings in this setting: