T wave oversensing
Tracing
Manufacturer Biotronik
Device PM
Field Sensing
N° 24
Patient
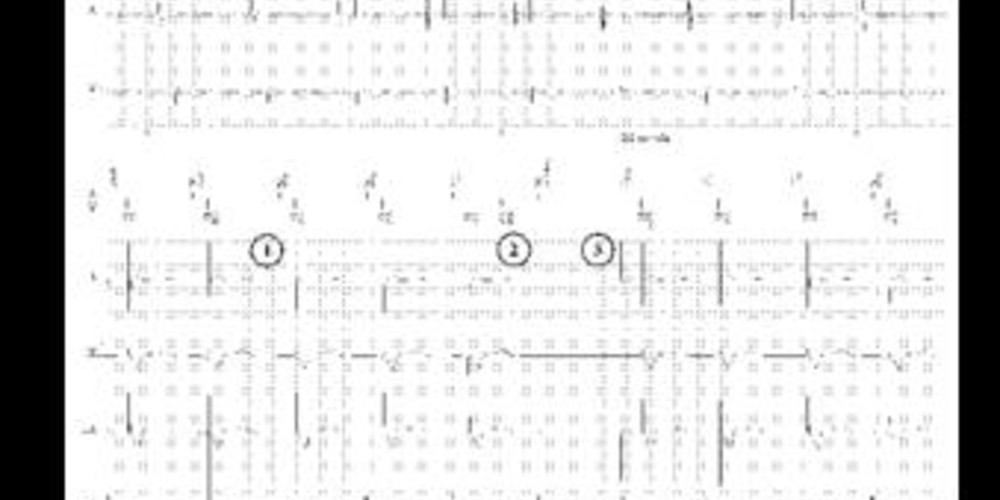
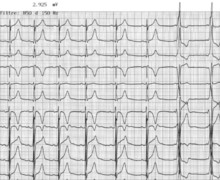
71-year-old man, implanted with a Biotronik Evia DR-T dual-chamber pacemaker for syncopal complete atrioventricular block; routine control; numerous PVCs recorded in the device's memory.
Graph and trace
- atrial sensing and ventricular pacing;
- ventricular pacing and T wave oversensing; sinus P wave sensed in the PVARP (prolongation of the post-PVC PVARP);
- atrial pacing and ventricular pacing.
Other articles that may be of interest to you


The quality of the sensing of a signal is dependent on a certain number of its physical characteristics:
This tracing reveals an oversensing of the T wave, the ventricular channel being too sensitive. Automatic and adaptive cycle-to-cycle sensing, which is absolutely essential for the proper functioning of a defibrillator, is now available in pacemaker platforms. Pacemaker constraints in terms of sensing of fast low-amplitude signals are less than those of a defibrillator (necessity to sense and treat ventricular fibrillation). On the other hand, the oversensing of a cardiac (T wave, P wave) or extracardiac (myopotential, interference, etc) signal can be extremely problematic in pacemaker-dependent patients. In the presence of T wave oversensing, as observed in this patient, programming of a fixed rather than automatic sensitivity may be preferred.