Single chamber discrimination: VT
Tracing
Manufacturer Abbott
Device ICD
Field Discrimination
N° 40
Patient
This 64-year-old man, presenting with ischemic cardiomyopathy and episodes of sustained VT, received a Abbott Atlas single chamber ICD for secondary prevention and was seen for a routine follow-up.
Main programmed parameters
- VF zone at 222 bpm and VT zone at 179 bpm
- Diagnosis required 8 cycles in the VF zone and 12 cycles in the VT zone
- Effective discrimination programmed in the VT zone
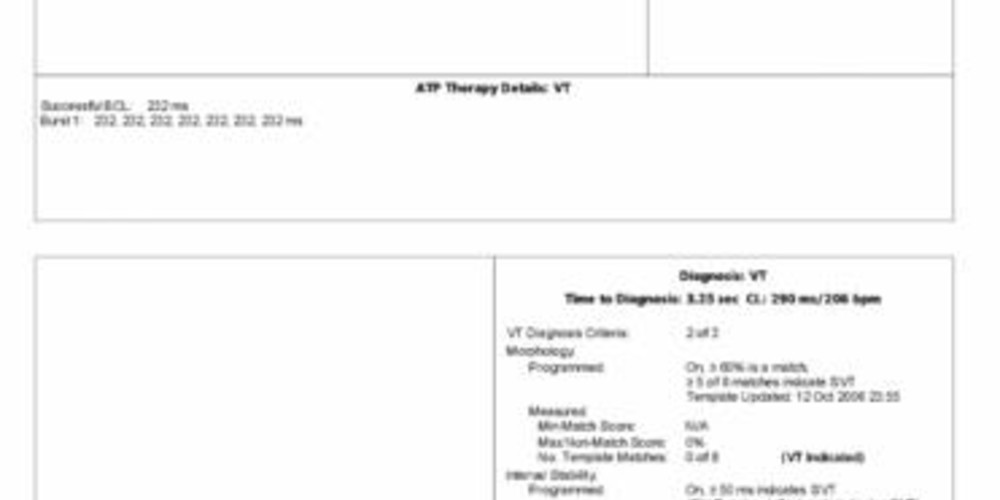
- VT diagnosis criteria: 2 out of 3
- Morphology: ON (60% 5 out of 8)
- Stability: ON 50 ms; detection window: 12 intervals
- Sinus interval history (SIH): passive; 2 intervals
- Sudden onset: ON, 80 ms
Graph and trace
Tracing
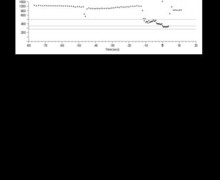
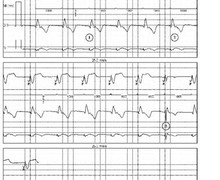
- spontaneous rhythm at 85 bpm;
- onset of tachycardia; the first cycles were not classified (non-concordance between instantaneous cycle and average of 4 preceding cycles: transitory rhythm);
- first cycle classified as T: the sudden onset of the tachycardia, obvious in this example, was analyzed from this first, pivotal cycle;
- VVI episode pacing mode after 4 cycles classified as T;
- diagnosis of VT after 12 cycles classified as T and discrimination in favor of VT. Stability was analyzed over the 12 cycles (in this example classified as T) preceding the diagnosis of VT. The shortest and longest cycles, which measured 281 and 297 ms, respectively, were not included in the analysis of stability. The second longest and second shortest cycles measured 285 and 297 ms, respectively, representing a stability of 12 ms (rounded to 10 ms in the narrative). In this example, morphology was analyzed over the 8 complexes that preceded the diagnosis of VT; in these 8 complexes, the 0 and x markers marked the absence of similarity with the reference morphology;
- burst of 8 stimuli;
- successful burst and diagnosis of return to sinus rhythm after 5 consecutive VS;
- analysis of ventricular complex morphology continues after the termination of VT, and is now similar to the reference ventricular complex (100, ν), confirming the proper function of this parameter.
Other articles that may be of interest to you


In the discrimination of the origin of arrhythmias, the single chamber defibrillators manufactured by St Jude Medical use 1) sudden onset, 2) rate stability associated with SIH, and 3) morphology of ventricular complexes. None of these parameters alone can flawlessly discriminate all tachycardias.
Each criterion may be programmed “ON”, “OFF” or “Passive”. The “Passive” mode allows an evaluation of a criterion’s performance without being included in the discrimination. When all criteria are on «Passive» or «OFF», discrimination is inactivated and therapy is delivered regardless of the tachycardia origin. Depending on the programming, each parameter may be more or less sensitive, or more or less specific.
In the majority of patients, the recommended programming is probably 2 out of 3 criteria. It is, however, recommended to program “All” criteria in the presence of atrial tachycardia or atrial flutter (sudden onset, stable rhythm and unchanged QRS). The greater the number of programmed criteria, the higher the specificity, which occurs at the cost of sensitivity.