

Traditional pacing modes
According to the amount of leads and the model of the implanted device, different pacing modes are programmable. The function of each mode, its advantages and disadvantages need to be familier to the responsable clinician in order to ensure a safe and optimized follow-up of the implanted patient.
Content
The international code
A combined approach between the north american and the british societies of pacing and electrophysiology (NASPE and BPEG) resulted in a international code (NBG) which describes the various pacemaker modes. The modes are identified by a 4 or 5 letter code which describes the basic functioning of the device.
- The first letter describes the site(s) of stimulation: ventricle (V), atrium (A), both atrium and ventricle (D), or none (O)
- The second letter describes the site(s) of sensing: the same letters as above.
- The third letter describes the function: inhibit (I), trigger (T), both/dual (D) or none of mentioned (0).
- The fourth letter describes whether rate response is active (R) or disabled (0).
- The fifth letter describes there is multisite pacing: absent (0), atrial (A), ventricular (V) or dual (D: A+V).
Single chamber pacing
Asynchronous modes SOO (VOO and AOO)
- Single chamber pacing
- No detection
- Asynchronous stimulation
The A00 and V00 modes deliver asynchronous stimulation at a fixed lower rate. The is no inhibition by intrinsic events in the designated chamber since there is no sensing.
The only programmable interval (rate) is the pacing rate (rate = 60.000 / stumation interval). It is the most basic pacing mode and was in fact the only pacing mode in the first pacemakers.
On the electrocardiogram during V00 mode we observe regular pacing spikes without interruption by intrinsic ventricular activity.
During A00 mode we will observe regular atrial pacing spikes without interruption by intrinsic atrial activity.
The A00 and V00 modes are the magnet modes for the single chamber atrial lead and ventricular lead pacemakers, respectively. The V00 mode is also the magnet mode of VDD mode pacemakers.
The S00 mode is nowadays obsolete for permanent programming and may be still used for testing; it may also be programmed in order to avoid detection of electromagnetic interference which may result in problematic inhibition in pacemaker dependent patients. Since there is a arrhythmogenic risk due to pacing in the vulnerable phase of the T-wave, it should only be used for testing purposes.
SSI/SSIR modes
The SSI mode is a single chamber mode, VVI when the lead is implanted in the ventricle and AAI when the lead is in the atrium. For these two pacing modes, a pacing stimulus follows after the lower pacing rate interval. When an intrinsic event is sensed, pacing is withheld (inhibited) and the lower rate interval resets.
VVI/VVIR mode
- Ventricular stimulation
- Ventricular sensing
- Ventricular sensed event (outside of refractory periods) inhibits stimulation.
VVI mode delivers ventricular pacing at the programmed lower pacing rate, with inhibition when intrisic ventricular events are sensed. Only the ventricle is sensed and after every sensed event, the lower pacing rate interval resets.
It is important to note that sensing of a ventricular event most often occurs after onset of ventricular activation (beginning of the QRS complex). This is most prominent in patients with a right bundle branch block, where sensing of the ventricle only occurs when the activation wavefront passes the lead cathode, positioned in the right ventricle.
The first part of the coupling interval, after sensing/stimulation, is associated with a refractory period when the pacemaker can not sense any event. Any event occuring during this period does not reset the lower rate interval. The refractory period is necessary to avoid double sensing of the same QRS complex (intrinsic or paced) or to avoid sensing of the T-wave. When an event is sensed after the refractory period, it will inhibit cardiac pacing.
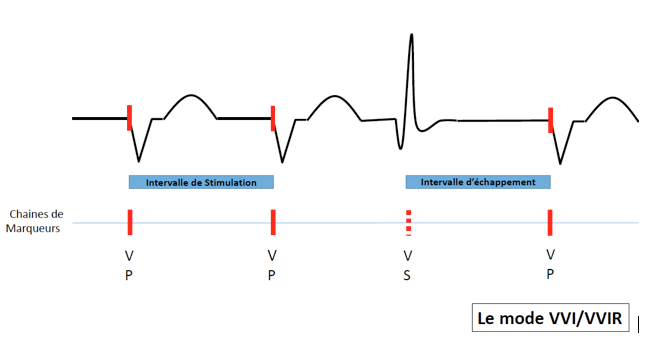
The VVIR mode is a single chamber ventricular pacing mode with rate response enabled. This means that the pacing rate is dependent on the activity of the patient as detected by a sensor.
VVI/VVIR mode is particularly indicated in patients with permanent atrial fibrillation where sensing of atrial events has no function. This mode may also be programmed in patients with paroxysmal episodes of bradycardia. The lower rate is then programmed lower than the intrinsic rate of the patient and the patient is only paced during episodes of pauses/bradycardia.
AAI/AAIR mode
- Atrial stimulation
- Atrial sensing
- Atrial events outside of refractory period will inhibit pacing.
AAI mode delivers atrial pacing at the programmed lower rate except when atrial events are sensed.
Sensing only occurs in the atrium.
Function is the same as for VVI mode. A higher sensitivity (lower sensitivity threshold) should be programmed, since the atrial events are most often of lower amplitude than ventricular complexes. The atrial refractory periodes should also be longer, to avoid sensing of ventricular events. The detection of R-wave by the an AAI pacemaker may result in a decrease of the actual lower pacing rate as each sensed R-wave resets the lower pacing rate interval. In case of far field oversensing of the R-wave, it is possible to make the pacemaker less sensitive and/or to extend the refractory period.
Typical ECG tracing during atrial pacing and capture with inhibiton during sensed intrinsic atrial activity.
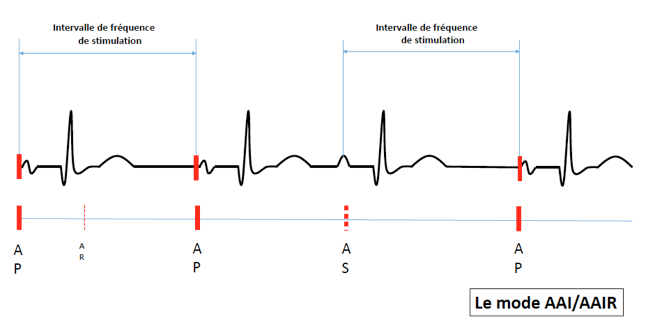
AAIR mode delivers atrial pacing with rate response.
The AAI/AAIR pacing mode is indicated in patients with sick sinus node disease with intact atrioventricular conduction. It is important to evaluate the quality of atrioventricular conduction. 1-to-1 atrioventricular conduction during fast atrial pacing (120-130 beats per minute) with normal PR-intervals and normal QRS complexes is a good sign of intact atrioventricular conduction. In this case, the risk of atrioventricular block is limited.
SST modes (VVT or AAT)
- Ventricular or atrial stimulation
- Ventricular or atrial sensing.
- Triggering of stimulation after sensed ventricular or atrial events outside of refractory periods.
In AAT and VVT modes, there is basic pacing at the programmed lower rate, but a sensed event triggers an immediate pacing stimulus in the corresponding chamber. This stimulation is not dangerous as it occurs in the natural refractory period.
The three parameters which are important to programme are the lower pacing rate, the maximal pacing rate and the refractory period. The latter parameters avoid rapid pacing.
On the surface ECG during VVT we observe: in absence of intrinsic atrial activity, ventricular stimulation and capture at a fixed rate. A sensed QRS complex triggers a pacing stimulus within the QRS complex. The QRS morphology therefore remains identical which is called pseudo-fusion or is slightly altered due to fusion between the intrinsic QRS complex and the paced QRS complex.
AAT mode is the same but then for the atrium.
Today, this pacing mode is rarely used. Pacing after detection is associated with increased and unnecessary battery drain. It may still be indicated in a small group of patients who have shown to experience oversensing, in these patients VVT/AAT mode may prevent inappropriate inhibition due to oversensed events.
Double chamber pacing
D00 mode
- Asynchronous dual chamber pacing
- Absence of sensing
D00 mode delivers sequential atrioventricular (AV) pacing at the lower pacing rate without inhibition by intrinsic activation.
The AV delays and VA delays are fixed and are not reset by sensed events since sensing is disabled.
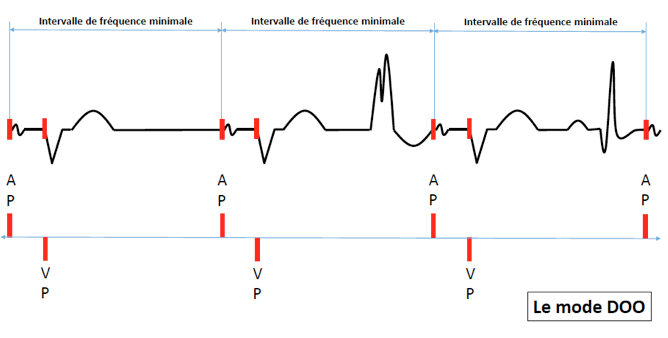
Besides being directly programmable, the dual chamber pacemaker will switch to D00 mode in case of magnet application (magnet mode, in exception of VDD mode which will switch to V00 mode).
DDD/DDDR mode
- Dual chamber stimulation (atrial and ventricular)
- Dual chamber sensing (atriale et ventriculaire)
- Dual response to detection (inhibition and triggering)
DDD mode is the standard programming option in dual chamber and resynchronization (with added left ventricular lead) therapy pacemakers. It enables maintanance of atrioventricular synchrony at rest but also during exercise when the intrinsic or paced atrial rate is elevated.
Intrinsic atrial activation occuring outside of refractory periods inhibits atrial stimulation. Intrinsic ventricular activation sensed outside of refractory periods inhibit ventricular stimulation.
Each stimulated atrial event or each detected atrial event outside the refractory periods marks the start of an AV delay and a minimum frequency interval.
The AV delays for sensed atrial events and paced atrial events are programmed seperately.. It is also possible to shorten the AV delay during higher heart rates (adaptable AV delay) or lengthen the AV delay to favour intrinsic atrioventricular conduction.
A paced ventricular complex may follow an instrinic atrial event a heart rates until the maximal tracking rate is reached. Above this limit the pacemaker is not allowed to pace the ventricles at the atrial rate.
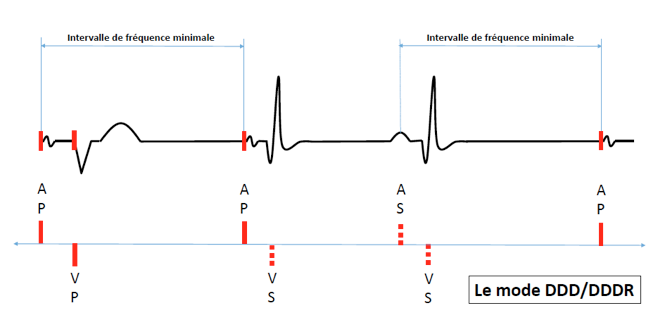
In DDDR mode, the pacemaker follows the fastest rate, being either the intrinsic atrial rate or the rate indicated by the sensor. The maximal tracking rate and the maximal sensor rate are to be programmed seperately.
The DDD mode is designed to respond to the characteristics presented by all implanted patients.
DDI/DDIR mode
- Dual stimulation (atrium and ventricle)
- Dual sensing (Atrial and ventricular)
- Inhibition of intrinsic events (atrial and ventricular)
Atrial stimulation occurs at the programmed lower pacing rate.
After atrial pacing, ventricular stimulation occurs following the AV delay when there is no ventricular sensed event during this delay.
A sensed atrial event inhibits atrial pacing and does not trigger an AV delay. When after a sensed atrial event, there is no intrinsic atrioventricular conduction, the pacemaker stimulates the ventricle at the programmed lower rate, such as during VVI mode.
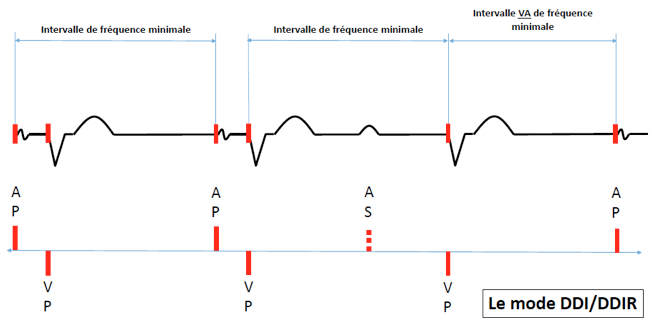
In case of atrial arrhythmia, there is no increase in ventricular pacing rate since sensed atrial events do not trigger an AV delay (no tracking).
The DDI mode is indicated in patients with frequent atrial arrhythmias such as in patients with brady-tachy syndrome. This pacing mode is not suitable for patients with complete AV block with elevated atrial rates since the atrial events do not trigger AV delays. DDI may be programmed in patients with complete AV block and sinus node dysfunction; in sinus rhythm we observe dual chamber stimulation; during atrial arrhythmia the fast atrial rates are not tracked. This mode is particularly useful when the mode switching algorithm functions suboptimally.
VDD mode
- Ventricular stimulation
- Dual chamber sensing (atrial and ventricular)
- Atrial sensing triggers ventricular stimulation with inhibition by both atrial and ventricular events.
Sensing occurs in the atrium and in the ventricle but pacing only occurs in the ventricle. The VDD mode delivers AV synchronized pacing. In absence of atrial sensed events, the pacemaker oprates as in VVI mode.
The ventricle is paced tracking the atrium until the maximal tracking rate is reached.
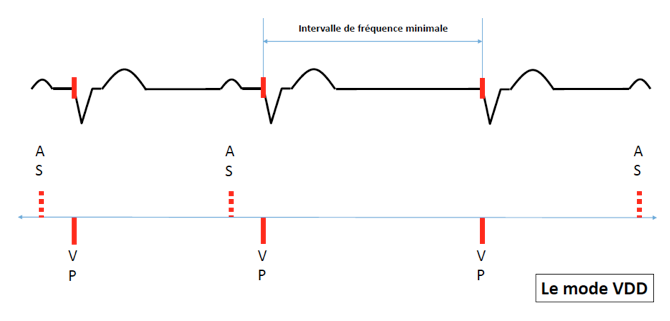
The VDD mode is thus not appropriate in patients with sick sinus syndrome as atrial back-up pacing is impossible. VDD mode is most appropriate for patients with complete AV block with normal sinus node function and normal chronotropic function. It is possible to deliver VDD mode using a single lead implanted in the ventricle with atrial electrodes floating in the atrium.
DDT mode
- Dual chamber stimulation (atrial and ventricular)
- Dual chamber sensing (atrial and ventricular)
- Dual chamber pacing triggered by any atrial or ventricular sensing.
This is a temporary testing mode used to test sensing.