ventricular AutoCaptureTM
Tracing
Manufacturer Abbott
Device PM
N° 15
Patient
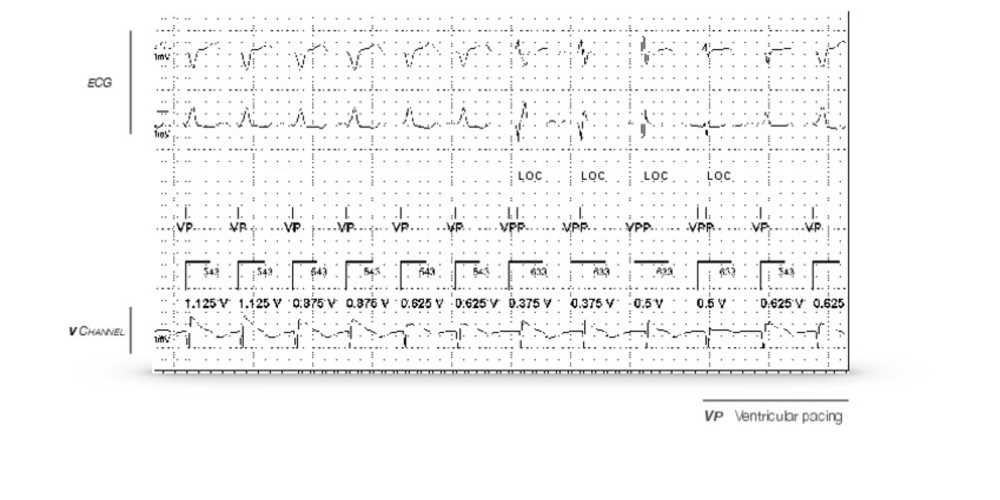
78-year-old man implanted with an AccentTM DR pacemaker for paroxysmal atrioventricular block; measurement of the right ventricular pacing threshold during the consultation.
Graph and trace
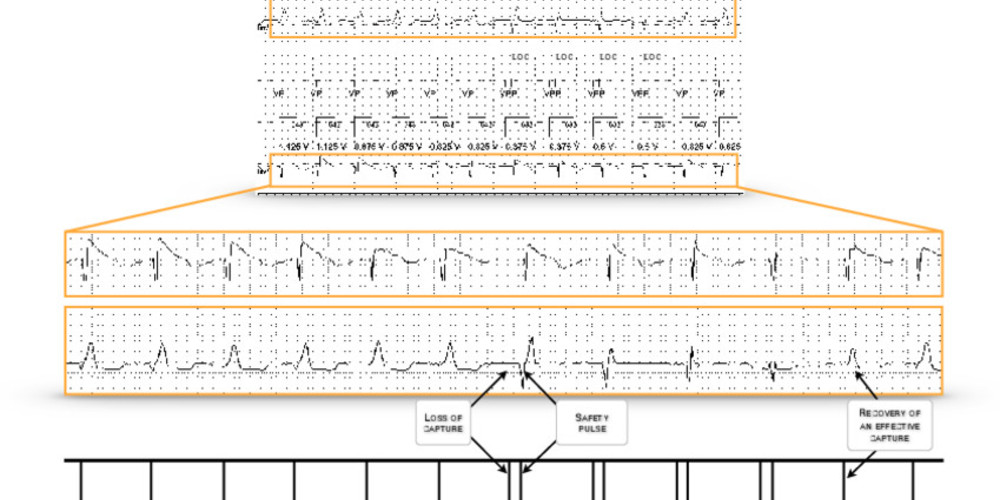
This is an automatic right ventricular pacing threshold measurement; initially, the pacing amplitude decreases in steps of 0.250 V every 2 cycles; up to 0.625 V, capture is effective; at the next step, the device diagnoses a loss of capture (LOC) and delivers a 5 V safety pulse (programmed pulse duration), 80 to 100 ms after the first noncapture; the device subsequently increases the amplitude in steps of 0.125 V; the pacing remains ineffective at 0.5 V with recovery of an effective capture at 0.625 V which corresponds to the threshold value.
Other articles that may be of interest to you


There is a long history of the use of ventricular AutoCaptureTM on St. Jude MedicalTM and AbbottTM pacemakers.
Certain key principles should be kept in mind: 1) for the older pacemakers (MicronyTM, VictoryTM and prior models), a bipolar ventricular lead was needed for programming ventricular AutoCaptureTM (bipolar sensing and unipolar pacing); for the newer devices, ventricular AutoCaptureTM can be activated regardless of the programmed sensing and pacing configurations;
2) an automatic AutocaptureTM setup test, used to verify the compatibility of the lead according to its polarization as well as to differentiate capture from capture failure, precedes the first activation of the device; this test remains optional (although recommended) before each threshold measurement; the use of ventricular AutoCaptureTM is only recommended when the amplitude of the polarization signal is less than 4 mV, when the safety margin between the amplitude of the evoked response signal and the sensitivity setting of the evoked response is at least 1.8 and when the safety margin between the amplitude of the polarization signal and the sensitivity setting of the evoked response is at least 1.7;
3) the automatic threshold measurement is based on the analysis of the evoked ventricular response;
4) the ventricular threshold is periodically measured at minimum every 8 to 24 hours (programmable value);
5) the ventricular pacing amplitude is automatically adjusted with a fixed and non-programmable safety margin of 0.25 V; this algorithm functions irrespectively of the programmed pulse duration;
6) the maximum delivered amplitude (outside of the backup pacing) is 4.5 V for the programmed pulse duration;
7) there is a cycle-to-cycle control of ventricular capture efficiency;
8) In the event of a loss of capture, a 5 V backup pulse is delivered 80 to 100 ms after the first stimulus.
There are 3 available settings for ventricular AutoCaptureTM:
1) Setup: this setting is available during the initial activation; the programmer then proposes to start the Setup test followed by the Pacing test if AutoCapture is recommended;
2) On: the device measures the threshold, automatically adjusts the pacing amplitude and records the threshold measurement in the Threshold Curve and stores the EGM corresponding to the last threshold;
3) Off: the device does not measure the pacing threshold and does not perform any automatic adjustment of the pulse amplitude.
The following settings are adjustable in the Auto Capture Settings window:
1) the configuration of the backup pulse which allows programming the polarity configuration of the backup safety pulse to the bipolar or unipolar mode (nominal value);
2) the search interval that programs the periodicity of the 8-hour (nominal value) or 24-hour threshold measurement;
3) the paced/sensed AV delays that determine the paced AV Delay and sensed AV Delay settings used during a threshold search to 50/25 ms (nominal value), 100/70 ms or 120/100 ms; the recommended setting for this parameter is 50/25 to prevent fusions; a fusion with intrinsic activation is more likely with longer programmed delays and can result in inaccurate threshold search results.