Vp-suppression and risk of pacemaker-mediated tachycardia
Tracing
Manufacturer Biotronik
Device PM
Field Pacing Modes
N° 4
Patient
- 83-year-old man
- Evia DR-T pacemaker (Biotronik) for paroxysmal third-degree atrioventricular block
- Vp-suppression
- Palpitations and recording of this tracing
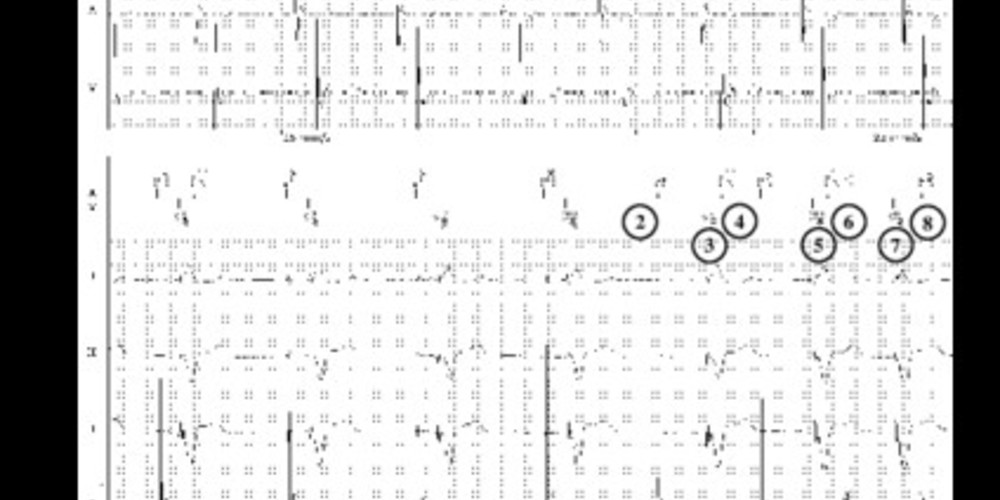
Graph and trace
- Atrial pacing and ventricular pacing (AP-VP)
- Programming of the Vp suppression (vertical line)
- Search for spontaneous conduction with prolongation of the AV delay to 450 ms
- Ventricular pacing with long AV delay
- Probable retrograde conduction sensed outside the refractory periods (AS)
- 8 cycles with AV delay at 450 ms; the search for atrioventricular conduction failed
- Prolonged AV delay so as not to exceed the synchronous maximum tracking rate
- Retrograde conduction
- PMT with adjustment of the AV delay so as not to exceed the maximum rate
- After 8 VP-AS cycles > 100 beats per minute, with stable VP-AS intervals and a VP-AS interval duration less than the programmed value, suspicion of PMT
- Prolongation of the AV delay over one cycle
- The prolongation of the AV delay leads to a prolongation of the AS-AS interval (the time of occurrence of the atrial activity is contingent on when the ventricle is paced)
- Prolongation of the PVARP for one cycle; the ensuing atrial activity falls within the PVARP and does not trigger an AV delay
- Termination of the tachycardia
Comments
- When the pacemaker operates in DDD mode, the search for spontaneous conduction is based on an atrioventricular delay hysteresis with an AV delay of 450 ms during 8 cycles
- There can be no dropped P waves during this search (if absence of spontaneous conduction, ventricular pacing after 450 ms)
- In patients with altered anterograde conduction but preserved retrograde conduction, prolonging the AV delay favors the occurrence of retrograde conduction which can generate a pacemaker-mediated tachycardia without the need for other triggering factors
- The number of PMT can be substantial
- The simplest and most logical approach in the presence of a permanent complete atrioventricular block is not to program the Vp suppression algorithm
- When the conduction disorder is paroxysmal and when it is deemed desirable to preserve the spontaneous conduction, it is therefore essential to verify that the PVARP is appropriately programmed longer than the retrograde conduction time
Other articles that may be of interest to you