Basic concepts
In standard practise, a VF-zone was conventionnaly programmed starting at 188-200 bpm with immediate high-energy shock as first therapy. Many ventricular arrhythmias, with short cycle lengths <320 ms and labeled as VF, actually are rapid monomorphic VTs. Concerns about lack of efficacy, risks of acceleration in life-threatening arrhythmias and syncope due to delay of therapy have precluded empirical programming of anti-tachycardia pacing in the VF zone. However, if cardioversion shocks are effective in interrupting fast monomorphic or polymorphic VTs, they are painful, drain the battery and overtreatment with ICD shocks is consistently associated with significant detrimental impact on patient mental and physical well-being. Reports of anxiety syndome, depression, and poor quality of life are common in patients affected by the occurrence of multiple painful shocks. Reducing shocks to improve quality-of-life scores, to decrease discomfort, pain and anxiety and to increase ICD acceptance now appears as a priority for optimal programming.
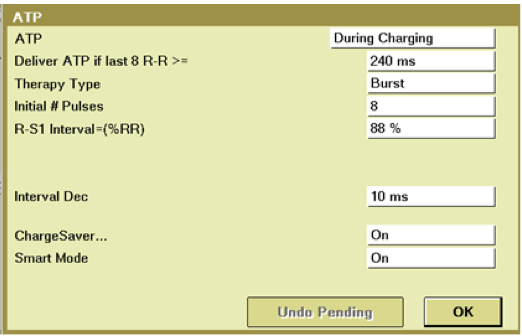
The PainFREE Rx II trial (a prospective, randomized, multicenter study) demonstrated that ATP was, with a single empirical ATP attempt (8 beats at 88%), highly effective in treating fast VT, significantly improving the quality of life and reducing the relative number of shocks without any clinical difference in episode duration, arrhythmic syncope, acceleration, or sudden death.
Anti-tachycardia pacing can be considered as safe and effective, promotes less pain and better quality of life, prolongs the battery longevity and therefore should be recommended as the first-line therapy for fast VT in the VF zone with a high chance of arrhythmia termination and minimal delay in therapies.
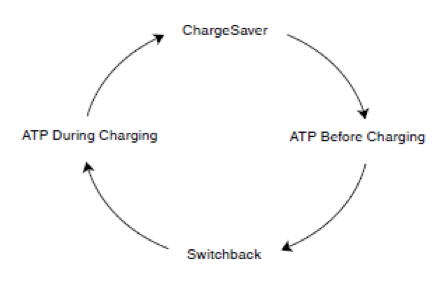
Subsequently, device manufacturers have developed algorithms with subtle specificities to deliver a limited number of ATP sequences before or during the charge in the VF zone. The major advantage of an ATP delivered during the charge is that it provides one attempt to interrupt the tachycardia without potentially delaying the shock if ATP fails to terminate the arrhythmia. In contrast, it causes battery depletion nearly equivalent to a shock. ATP delivered before the charge prevents battery depletion but there is in some specific patients a fine balance between the risk of excessive shocks and the risk of delaying therapies with potential clinical consequences and poor ability to tolerate ventricular arrhythmias. According to the manufacturer, there is a possible switch from ATP during charging to ATP before charging if burst pacing therapy successfully terminates the arrhythmia.
Multiple factors may affect the efficacy of ATP and may be programmed according to the manufacturers. Regarding optimal ATP programming for very fast VT, a burst (greater effectiveness and a lower incidence of acceleration with one burst over one ramp) with 8 to 15 beats (no superiority of a 8- versus 15-beats train), quite long cycle length (88% of the VT cycle length compared to shorter ones for slower VTs) and with left ventricular or biventricular pacing in patients implanted with a CRT device may improve efficacy.